 Chloramphenicol (CAP) is a naturally occurring, broad-spectrum antibiotic (Figure 1) that is artificially manufactured for use in veterinary and human medicine. Due to its adverse effects in humans, use of the antibiotic is restricted and, in some situations, prohibited. Increased legislation has led to the imposition of a ‘zero tolerance’ of CAP in food products by the European Council Regulation EEC No. 2377/90[1] and the technologies used in CAP detection being both improved and updated. A case study using the Bruker EVOQ™ Qube identifies CAP in milk matrix at 0.02 ppb, meeting the required minimum required performance level (MRPL) of 0.3 ppb.
Chloramphenicol (CAP) is a naturally occurring, broad-spectrum antibiotic (Figure 1) that is artificially manufactured for use in veterinary and human medicine. Due to its adverse effects in humans, use of the antibiotic is restricted and, in some situations, prohibited. Increased legislation has led to the imposition of a ‘zero tolerance’ of CAP in food products by the European Council Regulation EEC No. 2377/90[1] and the technologies used in CAP detection being both improved and updated. A case study using the Bruker EVOQ™ Qube identifies CAP in milk matrix at 0.02 ppb, meeting the required minimum required performance level (MRPL) of 0.3 ppb.
CAP is a bacteriostatic antimicrobial effective against both Gram-positive and -negative bacteria. CAP was first introduced into clinical practice as ‘chloromycetin’ in 1949, derived from the bacterium Streptomyces venezuelae. By inhibiting protein synthesis, CAP stops protein growth. It prevents protein chain elongation by inhibiting the ribosome, directly interfering with the substrate binding.
A very small, extremely lipophilic molecule, CAP remains relatively unbound to proteins. These physiochemical properties give it excellent blood-brain barrier permeability and make it the primary treatment for staphylococcal brain diseases. As one of the first antibiotics to be synthetically mass manufactured, CAP was used as a first line of typhoid treatment. In the EU today, CAP is often restricted to use with serious infections and only when necessary. However, the prescribing of CAP for the treatment of optical conditions and in topical preparations is still common. CAP is also still prescribed frequently in developing countries due to its inexpensive high availability. With a long drug history across a number of countries, CAP has around 40 trade names, including Cedoctine (Egypt, intravenous preparation), Edrumycetin 250 (Bangladesh, capsule) and Vanmycetin (Hong Kong, eye drops).
Chloramphenicol in Humans
The liver metabolizes CAP, enabling the kidneys to excrete the inactive metabolite out of the system. People with subnormal liver function, whether due to age or health, are susceptible to CAP accumulation. The half-life of CAP is between 1.5 and 4 hours in healthy adults, up to 10 hours in 10–16-day-old infants and may be in excess of 24 hours in neonates.[2] This makes infants the group at largest risk.
CAP can enter the food supply chain at a number of points. The first is due to its natural prevalence. CAP is a naturally occurring chemical produced by S. venezuelae, a Gram-positive filamentous Actinomycetes bacteria. Actinomycetes are found in soils across the world. Per hectare, the biomass of Actinomycetes is 400–5,000 kg in 15 cm of topsoil.[3]
Secondly, CAP is still prescribed to humans as topical preparations, particularly for the eyes for conditions such as bacterial conjunctivitis, but also when other medication is contraindicated. This means that CAP may become present in surface and wastewater as a contaminant type known as a pharmaceutical and personal care product. A study of organic antibiotic presence in surface waters and sewage plant effluent detected CAP at concentrations of 0.56 µg/L in sewage treatment plant effluent and 0.06 µg/L in surface water.[4]
Finally, plants absorb CAP from the soil and water.[5] If a food-producing animal drinks contaminated water, eats contaminated plants or is indeed treated illicitly with CAP, then the food it produces will also contain CAP.
Harmful Effects of CAP on Infants
There are several noted harmful effects of CAP on infants, whether that be through medication or the ingestion of contaminated food stuffs.
Gray baby syndrome is a potentially fatal reaction to CAP, occurring in premature and newborn infants. Because the liver enzymes of an infant are not fully developed, any CAP received across the placenta and or in breast milk remains unmetabolized in the body, inducing hypotension, hypothermia, flaccidity, cardiovascular collapse, cyanosis and death within hours.[6] Symptoms include blue-gray skin color, abdominal distension, failure to feed, vomiting and irregular breathing. A case study by Halveka and Frankova on the ‘Adverse effects of chloramphenicol in newborn infants’ looked at this in more detail.[7]
A Chinese study on children also showed a significant dose-response relationship between the risk of acute lymphocytic leukemia and acute non-lymphocytic leukemia with CAP treatment for more than 10 days. The risks associated being 11.0 and 12.0, respectively.[8]
Perhaps the most serious of all are blood dyscrasias and bone marrow suppression, such as idiosyncratic aplastic anemia and nonregenerative anemia. CAP has a direct toxic effect on human mitochondria, suppressing bone marrow and its production of red blood cells, white blood cells and platelets. Aplastic anemia is a rare but often fatal condition with no treatment.
As with any antimicrobial agent, CAP can disrupt the existing balance of gastrointestinal microbial flora, leading to an increase in those that are normally saprophytic. This can interfere with vitamin K production by intestinal bacteria and an overgrowth of Candida and Clostridium difficile, producing a toxin causing diarrhea and pseudomembranous colitis.
CAP may also have indications as a carcinogen in humans as reported by the International Agency for Research on Cancer,[9] although the evidence is noted as ‘limited.’
Current Legislation
In 1968, legislation was passed in the U.S., in line with the Food, Drug & Cosmetic Act of 1938, stressing the need for manufacturers to demonstrate their products were safe, with a particular emphasis for this to be observed with the regulation of animal drugs.[10]
The Center for Veterinary Medicine (CVM) never approved CAP to be used in the treatment of food-producing animals, as there was a fear the harmful residues would remain in the food products. A series of tests on U.S. meat samples in the 1980s demonstrated that potentially harmful residue levels of CAP were present. This indicated that veterinarians and farmers were still using the drug to treat animals illegally.[10]
In 1986, CAP was banned by the CVM for the treatment of pets to prevent it being passed on for the treatment of food-producing animals and was then banned by the EU for use in veterinary medicine in 1994. Subsequently, CAP is not found in food products from the EU or Americas, but low residue levels have been detected in imports of products such as milk, honey and shrimp from Asia. Many countries, such as the United States and those in the EU, prevent such foods from entering the country. The EU decision 2003/181/EC states that any detected level of CAP in milk is strictly prohibited and that methods used for CAP detection must meet or exceed the MRPL of 0.3 ppb.[11]
The China National People’s Congress passed the first law of its kind in Food Safety Law on February 28, 2009,[12] stipulating a ban on all non-approved chemicals and materials (including CAP) other than “those items proved to be safe and necessary in food production.”[13]
The Food Safety and Standards Authority of India (FSSAI) was established under the Food Safety and Standards Act of 2006, and has dedicated legislation regarding milk. Lab Manual 15, produced by FSSAI, gives a method for the determination of CAP in milk using high-pressure liquid chromatography (HPLC)-mass spectrometry (MS)/MS.[14]
Currently, the recommended method of detection for CAP is LC coupled to triple quadrupole MS (LC TQ-MS/MS). With one of the fastest sample-to-report times available as a result of its exception-based data review PACER software, the Bruker EVOQ™ is ideal for applications in food testing where time can be critical.
The EVOQ LC-TQ has a number of innovative features giving it sustained high sensitivity for robust results to meet the authorities requirements. The novel, vacuum-insulated probe (VIP)-heated ESI (VIP-HESI) prevents the degradation of thermally labile molecules, whereas the active exhaust prevent the recirculation of nebulized gasses, silencing much of the chemical noise. By utilizing an inter-laced quadrupole (IQ) dual ion funnel, Bruker’s EVOQ prevents signal roll-off while the orifice interfaced is continually flushed to keep it clean and eliminate the need for re-tuning.
The excellent levels of sensitivity and robustness offered by the Bruker EVOQ Qube™ make it easily capable of detecting substances, such as CAP, in complex matrices down to sub 0.1 ppb, far surpassing the MRPL of 0.3 ppb.
EVOQ Qube Case Study
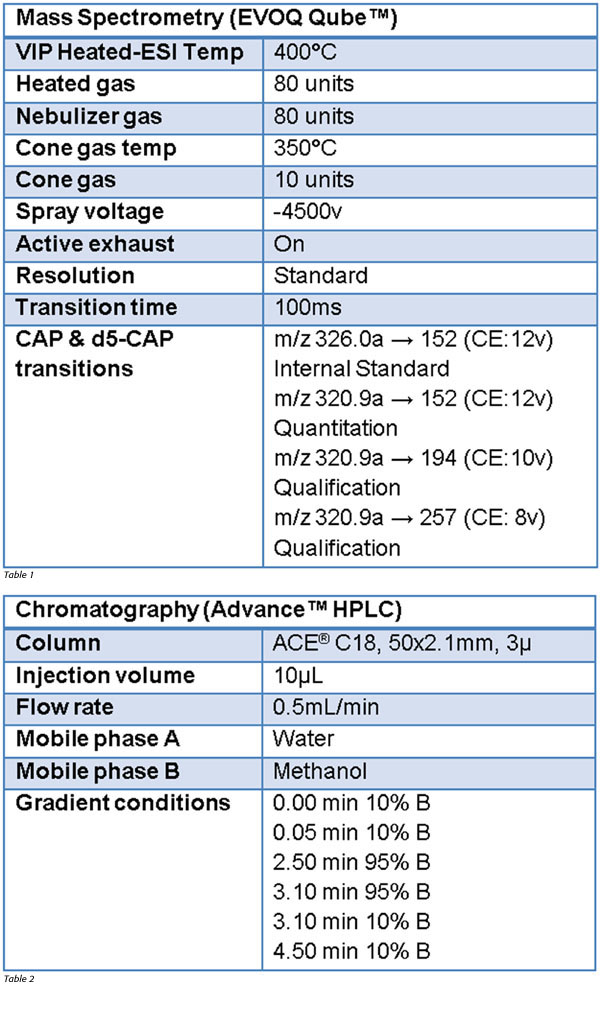 A blank milk matrix was prepared in accordance with the method stipulated in Cronly et al.[15] through the addition of 1 mL acetonitrile and 0.25 g NaCl to whole milk. The slurry was centrifuged, and the top organic layer transferred to a separate centrifuge tube. This was then evaporated to dryness at 45 °C and reconstituted in 0.5 mL initial mobile phase (90:10 Water:MeOH).[16] The resulting mixture was filtered through a 0.2-µm PVDF syringe filter and varying amounts of CAP (98%) was added to aliquots of this milk matrix along with 0.3 ppb (in matrix) d5-CAP (100 μg/mL in acetonitrile) as an internal standard. The instrument calibrations are shown in Tables 1 and 2.
A blank milk matrix was prepared in accordance with the method stipulated in Cronly et al.[15] through the addition of 1 mL acetonitrile and 0.25 g NaCl to whole milk. The slurry was centrifuged, and the top organic layer transferred to a separate centrifuge tube. This was then evaporated to dryness at 45 °C and reconstituted in 0.5 mL initial mobile phase (90:10 Water:MeOH).[16] The resulting mixture was filtered through a 0.2-µm PVDF syringe filter and varying amounts of CAP (98%) was added to aliquots of this milk matrix along with 0.3 ppb (in matrix) d5-CAP (100 μg/mL in acetonitrile) as an internal standard. The instrument calibrations are shown in Tables 1 and 2.
As a consequence of CAP being classified as a forbidden Group A substance, Decision 2002/657/EC specifies parameters and a minimum of four identification points (IPs) to confirm detection.[17] This was undertaken with two multiple reaction-monitoring assays (MRMs) with 1.0 IP assigned for the precursor ion and 1.5 IPs assigned for each transition product, provided that the ion ration for each MRM matches the certified reference material within tolerances, for example, for qualification MRMs with ion ratios between 20% and 50% of the most intense transition, the maximum permitted tolerance is ±25%. In the current analysis, the ion ratios were found to be consistent (<10% relative SD) from 0.05 ppb to 1 ppb levels.
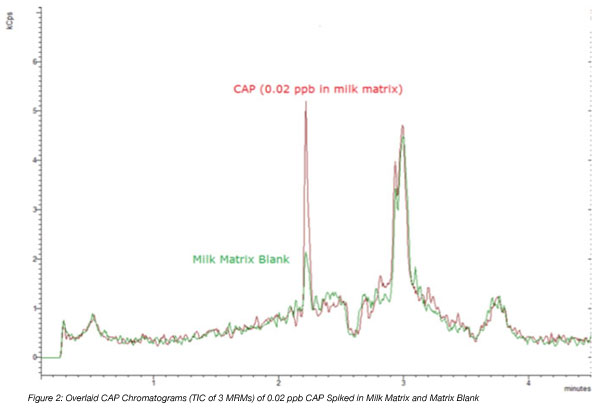 The overlaid chromatograms of the blank matrix and that with the lowest spike (0.02) are shown in Figure 2. Although a small amount of chemical noise was picked up, the spiked sample showed a significantly higher reading indicating a clear detection of CAP at 0.02 ppb.
The overlaid chromatograms of the blank matrix and that with the lowest spike (0.02) are shown in Figure 2. Although a small amount of chemical noise was picked up, the spiked sample showed a significantly higher reading indicating a clear detection of CAP at 0.02 ppb.
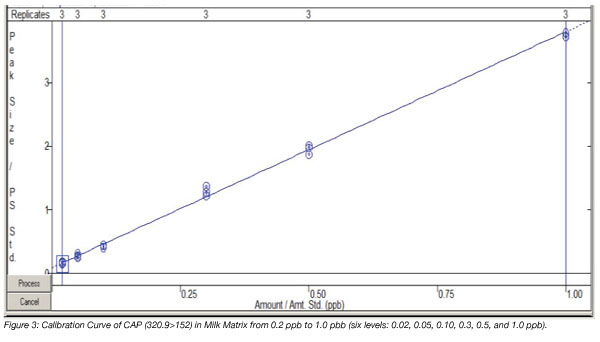
A six-level matrix matched calibration curve from 0.020 to 1.0 ppb was generated with each level analyzed in triplicate (Figure 3). Excellent linearity was obtained with R2=0.9980 (weighting factor =1/×).
Conclusions
With food legislation constantly under review to combat the very real risk of food contamination, it is becoming more and more difficult for food testing laboratories to meet the specifications set down by the authorities. The high risk of infants suffering due to exposure to CAP has pushed identification of CAP in milk to the forefront. The Bruker EVOQ Qube can quickly and accurately analyze milk matrices using LC-MS/MS for trace amounts of CAP. Being able to quantify concentrations as low as 0.02 ppb means it easily meets the requirements set by many authorities for the MRPL of 0.3 ppb.
Mauricio Splendore, Chris Kellogg and Rohan Thakur are members of the Bruker CAM Division, Fremont, CA.
References
1. Council Regulation (EEC) No. 2377/90 of June 26, 1990 (August 18, 1990), Laying down a community procedure to set up a maximum residue lmits of veterinary medicinal products in food stuffs of animal origin. Official J EU L224:1–8.
2. www.rxmed.com/b.main/b2.pharmaceutical/b2.1.monographs/CPS-%20Monographs/CPS-%20(General%20Monographs-%20C)/CHLORAMPHENICOL.html.
3. Brady, N.C. and R.R. Weil. 2002. The nature and properties of soils. 13th edn.
4. Hirsch, R., T. Ternes, K. Haberer and K.-L. Kratz. 1999. Occurrence of antibiotics in the environment. Sci Total Environ 225:109–118.
5. Berendsen, B. et al. 2010. Evidence of natural occurrence of the banned antibiotic chloramphenicol in herbs and grass. Anal Bioanal Chem 397:1955–1963.
6. McIntyre, J. and I. Choonara. 2004. Drug toxicity in the neonate. Biol Neonate 86:218–221.
7. Havelka, J. and A. Frankova. 1972. Adverse effects of chloramphenicol in newborn infants. Cesk Pediatr 27:31–33.
8. Ou Shu, X. et al. 1987. Chloramphenicol use and childhood leukemia in Shanghai. Lancet 330:934–937.
9. monographs.iarc.fr/ENG/Monographs/suppl7/Suppl7-41.pdf.
10. www.fda.gov/AboutFDA/WhatWeDo/History/ProductRegulation/AnimalHealthandConsumerProtection/default.htm.
11. http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2003:071:0017:0018:EN:PDF.
12. www.fas.usda.gov/gainfiles/200903/146327461.pdf.
13. www.chinadaily.com.cn/language_tips/2009npc/2009-02/28/content_7525363.htm.
14. fssai.gov.in/Portals/0/Pdf/15Manuals/ANTIBIOTICS%20AND%20RESIDUES.pdf.
15. Cronly, M. et al. 2010. Rapid multi-class multi-residue method for the confirmation of chloramphenicol and eleven nitroimidazoles in milk and honey by liquid chromatography-tandem mass spectrometry (LC-MS). Food Addit Contam Part A Chem Anal Control Expo Risk Assess 27:1233–1246
16. Application Note #704422. 2012. Quantitative analysis of chloramphenicol in milk using EVOQ™ Qube triple quadrupole mass spectrometer. Bruker Chemical and Applied Markets Division (CAM), Fremont, U.S.
17. eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2002:221:0008:0036:EN:PDF.
The Danger of Chloramphenicol in Milk



