
According to recent data from the U.S. Centers for Disease Control and Prevention (CDC), more than 60 percent of all the reported foodborne disease outbreaks in the United States are attributed to retail foodservice establishments.[1] As reported previously, failures to handle and prepare food safely in these establishments are the primary contributing factors that lead to foodborne disease outbreaks. The majority of the food safety hazards that exist in these establishments and their related probability of occurrence are well-known. According to the U.S. Food and Drug Administration (FDA) and CDC, the top five risk factors that contribute to the most foodborne disease outbreaks in foodservice establishments are:
1. Improper hot/cold holding temperatures of potentially hazardous foods
2. Improper cooking temperatures of food
3. Contaminated utensils and equipment
4. Poor personal hygiene
5. Food from unsafe sources
Scientific studies have also validated these factors, and there is continual evidence that the lack of their control leads directly to foodborne disease outbreaks from retail foodservice establishments.[2] One scientific study showed that certain local health department inspection violations (each related to the top-five risk factors) were more likely to be associated with restaurants that had actually caused foodborne disease outbreaks in Minnesota.[3] When the authors compared these violations with contributing factors of foodborne illness as defined by CDC,[4] they found that about two-thirds of the top violations observed during inspections at restaurants associated with outbreaks fell into the ‘‘contamination’’ category—for example, contamination of hands, surfaces, and food.
Why No Bare-Hand Contact?
Contamination of foods via the hands ranks highly among the contributing factors identified during outbreak investigations. In a report on the factors contributing to foodborne disease outbreaks from 1998 to 2002,[5] bare-hand contact, inadequate cleaning of processing or preparation equipment or utensils, and handling of food by an infected person or an asymptomatic carrier were among the most important factors (associated with 26%, 25%, and 22% of disease outbreaks, respectively). Foodborne pathogens with low infective doses may be present on hands in high numbers and can be easily transferred to foods, food contact, and nonfood contact surfaces, necessitating barriers to transmission.[6–8]
According to FDA, when hands are contaminated or soiled, effective hand hygiene (HH) practices may not be sufficient to prevent the transmission of transient pathogens from the hands to ready-to-eat (RTE) foods.[9] The 2017 FDA Food Code discourages bare-hand contact with RTE food and recommends the use of suitable utensils, deli tissues, single-use gloves, or dispensing equipment when handling these food items.[10] The majority of individual state food codes have adopted and enforce this rule.[11] The obvious objective in utilizing gloves in foodservice is to minimize physical, chemical, and microbiological contamination of food. Gloves can unfortunately offer a false sense of security both on the part of food workers and food safety managers when employees are not trained and glove use is not supervised properly.[12]
Improper Glove Use Increases Risk of Foodborne Disease Outbreaks
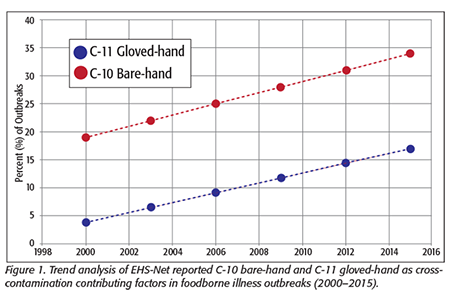 Although gloves (single-use and reusable) can be an effective tool to prevent cross-contamination of RTE foods from hands, improver glove use can actually increase this risk. In studies by the CDC Environmental Health Service (EHS-Net) and others between 2006 and 2016, around 16 percent of foodborne outbreaks implicated contaminated gloves or glove cross-contamination as a contributory cause.[13–17] A trend analysis of both gloved- and bare-hand contact, implicated as contributing factors from the time that glove rules were set into effect across the U.S. (2000–2015), shows a steady rise in percentages for both modes of cross-contamination.[18] Bare-hand contact was shown to be 15–18 percent higher (Figure 1). Taking model simulation results into consideration, a predictive cause for glove cross-contamination is quite likely on its way toward 20 percent or higher, based on the degree of variability and uncertainty presented by the data involved.[10] Trend analysis for the period from 2000 to 2015 and probably beyond indicates that current glove-use patterns, limitations, and relaxation of no-bare-hand contact rules (the “glove mandate”) due to glove failures could result in increasing numbers of foodborne illness outbreaks caused by gloves or glove cross-contamination. Affecting this would be improved glove types and management approaches designed to reduce cross-contamination risks.
Although gloves (single-use and reusable) can be an effective tool to prevent cross-contamination of RTE foods from hands, improver glove use can actually increase this risk. In studies by the CDC Environmental Health Service (EHS-Net) and others between 2006 and 2016, around 16 percent of foodborne outbreaks implicated contaminated gloves or glove cross-contamination as a contributory cause.[13–17] A trend analysis of both gloved- and bare-hand contact, implicated as contributing factors from the time that glove rules were set into effect across the U.S. (2000–2015), shows a steady rise in percentages for both modes of cross-contamination.[18] Bare-hand contact was shown to be 15–18 percent higher (Figure 1). Taking model simulation results into consideration, a predictive cause for glove cross-contamination is quite likely on its way toward 20 percent or higher, based on the degree of variability and uncertainty presented by the data involved.[10] Trend analysis for the period from 2000 to 2015 and probably beyond indicates that current glove-use patterns, limitations, and relaxation of no-bare-hand contact rules (the “glove mandate”) due to glove failures could result in increasing numbers of foodborne illness outbreaks caused by gloves or glove cross-contamination. Affecting this would be improved glove types and management approaches designed to reduce cross-contamination risks.
 The highest-risk glove/hand cross-contamination activity occurs when the same gloves are used to handle contaminated raw protein, then the employee touches food contact and nonfood contact surfaces (Figure 2), resulting in cross-contamination of food.[19] When food handlers touch raw proteins like chicken or ground beef and then touch other surfaces in the same kitchen, they can spread foodborne disease pathogens to these surfaces, where they can be “picked up” by the hands (with and without gloves) of other food handlers. Likewise, when a food handler switches tasks between handling raw and RTE foods and changes their gloves without washing their hands and forearms properly, they will contaminate the new pair of gloves because they have to touch the gloves to put them on. This can be a significant means of cross-contamination of RTE foods.[20]
The highest-risk glove/hand cross-contamination activity occurs when the same gloves are used to handle contaminated raw protein, then the employee touches food contact and nonfood contact surfaces (Figure 2), resulting in cross-contamination of food.[19] When food handlers touch raw proteins like chicken or ground beef and then touch other surfaces in the same kitchen, they can spread foodborne disease pathogens to these surfaces, where they can be “picked up” by the hands (with and without gloves) of other food handlers. Likewise, when a food handler switches tasks between handling raw and RTE foods and changes their gloves without washing their hands and forearms properly, they will contaminate the new pair of gloves because they have to touch the gloves to put them on. This can be a significant means of cross-contamination of RTE foods.[20]
In a study of 18 independent delicatessen operations, widespread microbial contamination (Escherichia coli, Staphylococcus aureus) was found on turkey, cream cheese, lettuce, and food contact surfaces.[21] A subsequent review of health inspection observations revealed that there was 1) inadequate HH, 2) no gloves used, 3) improper single-glove use, and 4) inadequate glove changes in 39 percent, 33 percent, 28 percent, and 67 percent of these delis inspected.[13] Other glove-use behaviors have been identified that cause cross-contamination when gloves are worn for long periods of food prep and not changed when punctured or contaminated.[21–23] Additionally, pathogens can be found to adhere better to the surface of gloves worn by food employees when gloves fit poorly or are not changed regularly.[24–28]
The use of gloves does not reduce the need to ensure proper handwashing before and after glove use. Because hands, like other surfaces, can become coated with oils, grease, and fats, for example, they should be both cleaned and sanitized, just as a food contact surface is cleaned and sanitized. This is especially important during use of foodservice gloves. The effective use of gloves depends on selection of the right glove type and maintenance of the glove barrier integrity. Undetected glove microperforations are a frequent occurrence. Microorganisms penetrate gloves via the microperforations under conditions of normal use. Puncture occurrence is directly related to duration of wearing and puncture hazards of procedures. With the interior of gloves presenting a warm, moist environment for microbial growth,[29] it is easy to understand why glove leaks would double cross-contamination risk. Handwashing is an important first step before every glove use, but preventing glove leaks is critical to ensure the final barrier between hands and foods is maintained because even with a prior handwash, interior glove counts of bacteria can be more than a million organisms.[30]
A glove puncture has been described as a “liquid bridge” of microbial contamination that can flow to food contact surfaces and foods.[31,32] Studies have shown that thousands of Staphylococcus bacteria can pass through a single glove hole during a 20-minute period, even though the hands were scrubbed prior to gloving.[9] Likewise, excess moisture buildup can release microbial contamination present in the difficult-to-clean fingernail regions that can then be spread all over the hand within the glove.[12,33–35] Leaks don’t just go in one direction out of the glove; they can also lead to permeation of microbial species, food debris, and chemical residues into the glove interior, leading to an increase in microbial load and chemicals that can then be released onto food and food contact surfaces.[36,37] This emphasizes the need to wash hands when they become contaminated with these soils, sometimes both before and after glove use.[12,38,39] Facility sanitizer chemicals, alcohol-based hand sanitizers (some but not all), or extreme temperature exposure can weaken glove material integrity[36,39,40] and thus, under conditions of use, should be monitored as part of the food safety management systems (FSMSs) outlined below.
Importance of FSMSs
The best means to prevent cross-contamination of foods is to ensure that all food contact surfaces are deep-cleaned and sanitized before food preparation, raw animal food prep is separated from RTE food prep, food handlers wash and sanitize their hands before glove use and do not handle RTE foods with bare hands, and the establishment has a monitoring and corrective action management system based on process Hazard Analysis and Critical Control Points (HACCP) principles to achieve active managerial control of cross-contamination.[41–43]
A FSMS to manage single-use gloves (a glove-use management system) employed along with handwashing can be an effective means to decrease the transfer of foodborne pathogens from the hands to food contact and nonfood contact surfaces and to food.[43]
A glove-use management system can be developed to include:
• Choice of the correct glove that with a specific glove-change frequency and type of foods prepared will minimize the risks related to undetected punctures
• Different-colored gloves for when employees handle/prep raw animal proteins versus RTE foods to provide a visual cue to managers for proper glove use and reduction of cross-contamination of food contact and nonfood contact surfaces from gloves
• Suggested raw animal protein-handling glove colors:
- Yellow: raw poultry (chicken, turkey, etc.)
- Red: raw meats (beef, pork, etc.)
- Pink: raw seafood
- Green: raw produce
• RTE foods glove colors:
- Clear, blue, or purple: all foods that will not undergo a kill or wash step to remove foodborne disease pathogens; use of colored gloves can provide a safety indicator to aid in preventing glove parts’ ending up in food products[4]
• A requirement to clean (wash) and sanitize hands before glove use to reduce pathogens on hands
• Manager training to enable visual monitoring of food handler tasks requiring separation of raw and RTE food handling
• This provides managers with a corrective action step to instruct the employee to stop food handling and induce a clean/sanitize procedure of surfaces when gloves are improperly used, which induces food handlers to always wear proper gloves.
• Monitoring can consist of determining numbers of gloves utilized by food handlers per unit time or glove discards in trash receptacles.[12,13]
• Compliance with this cross-contamination prevention can quickly be measured via third-party audits and via self-assessment systems like process HACCP.[41–43]
• Food handler training to include the practice of wearing the color-indicator gloves and to remove the gloves before they touch other surfaces or differentfood (which includes a handwash step between switching tasks)
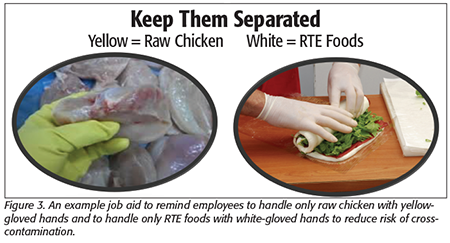 • Job aids to reinforce the proper glove use according to the glove-use management system (Figure 3)
• Job aids to reinforce the proper glove use according to the glove-use management system (Figure 3)
The Value Proposition for Retail Foodservice and Sales Businesses Using Gloves
Reducing the risk of a foodborne disease outbreak due to improper glove use can occur when only a single glove color is used to handle all foods (RTE and raw proteins) as well as all other tasks such as handling and emptying trash, cleaning equipment and facilities, cleaning rest rooms, washing dishes, cleaning up bodily fluids, etc. Managing proper glove use lets employees see (i.e., your food safety culture) gloves as a means to protect foods from cross-contamination.
Implementing and using a glove-use FSMS will change the business’s food safety culture within a retail sales or foodservice business by establishing the proper perspective of cross-contamination prevention by food handlers when wearing gloves (e.g., recognizing when hands are probably contaminated and what not to touch when gloved hands are contaminated with raw animal protein).
Improved health department compliance occurs where gloves are required by state food code rules. The majority of the 50 states have adopted, and now enforce, the 2005 or later FDA Food Code. The 2017 FDA Food Code requires gloves to be used by food handlers when preparing RTE foods.
Another value of implementing a glove-use management system is that the enhancement of compliance to prevent cross-contamination can be more easily monitored (by observations of proper glove use) by management and observed during health department inspections. For example, a manager or a health inspector can quickly see if a food handler is handling food safely while watching food prep and glove use (including handwashing most importantly before but also after gloves are used).
Customer experience can be enhanced in retail foodservice establishments where customers see food preparation by food handlers (e.g., the business can promote its food safety program showing how they use different-colored gloves to handle raw and RTE foods). This promotes customer understanding of how a retail establishment ensures raw food soils and associated contamination are “contained in the kitchen or back of the house.”
The authors would like to thank Lynda Ronaldson and Steve Ardagh of the glove company Eagle Protect PBC for their support in the collection of some of the raw scientific information and data analysis related to glove cross-contamination as a contributing factor in foodborne illness outbreaks.
Hal King, Ph.D., is CEO, Public Health Innovations LLC, www.publichealthinnovations.biz, and a member of the Editorial Advisory Board of Food Safety Magazine. He can be reached at halking@pubhealthinnovations.com. Barry Michaels, B.Sc., is an independent consultant and a partner in the B. Michaels Group Inc., an international scientific consultancy organization.
References
1. CDC. Surveillance for Foodborne Disease Outbreaks, United States, 2016, Annual Report (Atlanta: U.S. Department of Health and Human Services, CDC, 2018).
2. Hedberg, CW. 2013. “Explaining the Risk of Foodborne Illness Associated with Restaurants: The Environmental Health Specialists Network (EHS-Net).” J Food Prot 76:2124–2125.
3. Petran, RL, et al. 2012. “Health Department Inspection Criteria More Likely to Be Associated with Outbreak Restaurants in Minnesota.” J Food Prot 75:2007–2015.
4. Lynch, M, et al. 2006. “Surveillance for Foodborne-Disease Outbreaks—United States, 1998–2002.” Morb Mortal Wkly Rep 55:1–42.
5. CDC. 2006. “Surveillance for Foodborne Disease Outbreaks—United States, 1998–2002.” Morb Mortal Wkly Rep 55(SS10):1–34.
6. Todd, ECD, et al. 2008. “Outbreaks Where Food Workers Have Been Implicated in the Spread of Foodborne Disease. Part 4. Infective Doses and Pathogen Carriage.” J Food Prot 71:2339–2373.
7. Todd, ECD, et al. 2008. “Outbreaks Where Food Workers Have Been Implicated in the Spread of Foodborne Disease. Part 5. Sources of Contamination and Pathogen Excretion from Infected Persons.” J Food Prot 71:2582–2595.
8. Todd, ECD, et al. 2010. “Outbreaks Where Food Workers Have Been Implicated in the Spread of Foodborne Disease. Part 8.1. Gloves as Barriers to Prevent Contamination of Food by Workers.” J Food Prot 73:1762–1773.
9. citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.410.843&rep=rep1&type=pdf.
10. www.fda.gov/food/fda-food-code/food-code-2017.
11. Kambhampati, A, et al. 2016. “A State by State Assessment of Food Service Regulations for the Prevention of Norovirus Outbreaks.” J Food Prot 79(9):1527–1536.
12. Valero, A, et al. Chapter 2, “Risk Factors Influencing Microbial Contamination in Food Service Centres.” In Significance, Prevention and Control of Food Related Diseases (IntechOpen, DOI: 10.5772/63029, 2016).
13. Gould, LH, et al. 2013. “Contributing Factors in Restaurant-Associated Foodborne Disease Outbreaks, FoodNet Sites, 2006 and 2007.” J Food Prot 76(11):1824–1828.
14. ga.foodprotectiontaskforce.com/ga/assets/File/Delea_CDC Tools.pdf.
15. www.cdc.gov/nceh/ehs/nears/docs/2014-summary-report.pdf.
16. www.foodprotect.org/media/reportdate/cdc-report-compressed.pdf.
17. www.cdc.gov/mmwr/volumes/68/ss/ss6801a1.htm.
18. Michaels, BS, et al. “Hand & Glove Surface Cross-Contamination Potential Based on Nitrile and Vinyl Glove Surface Characteristics.” Presented at the IAFP Annual Meeting, Louisville, Kentucky, 2019.
19. Perez-Rodriguez, F, et al. 2006. “Linking Quantitative Exposure Assessment and Risk Management Using the Food Safety Objective Concept: An Example with Listeria monocytogenes in Different Cross-Contamination Scenarios. J Food Prot 69(10):2384–2394.
20. Lues, JFR and I van Tonder. 2007. “The Occurrence of Indicator Bacteria on Hands and Aprons of Food Handlers in the Delicatessen Sections of a Retail Group.” Food Control 18(4):326–332.
21. Murray, D, et al. 2013. “An Exploratory Study of Food Safety and Food Handling; Examining Ready-To-Eat Foods in Independent Delicatessen Operations.” Adv Biosci Biotechnol 4:430–436.
22. Ivanek, R, et al. 2004. “Mathematical Model of Listeria monocytogenes Cross-Contamination in a Fish Processing Plant.” J Food Prot 67(12):2688–2697.
23. Schaffner, DW. 2004. “Mathematical Frameworks for Modeling Listeria Cross-Contamination in Food-Processing Plants.” J Food Sci 69:R155–R159.
24. Michaels, B and E Todd. Chapter 5, “Food Worker Personal Hygiene Requirements during Harvesting, Processing and Packaging of Plant Products.” In Microbial Hazard Identification in Fresh Fruit and Vegetables, ed., J. James
(Hoboken, NJ: John Wiley & Sons, 2006).
25. Gill, GO and T Jones. 2002. “Effects of Wearing Knitted or Rubber Gloves on the Transfer of Escherichia coli between Hands and Meat.” J Food Prot 65:1045–1048.
26. Thimothe, J, et al. 2002. “Detection of Listeria in Crawfish Processing Plants and in Raw, Whole Crawfish and Processed Crawfish (Procambarus spp.).” J Food Prot 65(11):1735–1739.
27. Thimothe, J, et al. 2004. “Tracking of Listeria monocytogenes in Smoked Fish Processing Plants.” J Food Prot 67(2):328–341.
28. Dass, SC, et al. 2018. “Food Processing Environment Surveillance Using Amplicon Metagenomics: Assessing the Change in the Microbiome of a Fluid Milk Processing Facility before and after Cleaning.” BAOJ Food Sci & Tec 2:12.
29. Aycicek, H, et al. 2004. “Assessment of the Bacterial Contamination on Hands of Hospital Food Handlers.” Food Control 15(4):253–259.
30. Fendler, EJ, et al. 1998. “Handwashing and Gloving for Food Protection Part II.” Dairy Food Environ Sanitation 18:824–829.
31. Cole, WR and HR Bernard. 1964. “Inadequacies of Present Methods of Surgical Skin Preparation.” Arch Surg 89:215–222.
32. Fox, A. Hygiene and Food Production (Edinburgh and London: Churchill Livingstone, 1971).
33. Michaels, B and T Ayers. “Hazard Analysis of the Personal Hygiene Process. Proceedings of the 2nd National Sanitation Foundation International Conference on Food Safety, Savannah, GA, 2000.
34. Michaels, B. 2001. “Are Gloves the Answer?” Dairy Food Environ Sanitation 21(6):489–492.
35. Lin, CM, et al. 2004. “Comparison of Hand Washing Techniques to Remove Escherichia coli and Calicivirus Under Natural or Artificial Fingernails.” J Food Prot 66(12):2296–2301.
36. www.food-safety.com/magazine-archive1/junejuly-2004/understanding-the-glove-risk-paradigm-part-i/.
37. Wallemacq, PE, et al. 2006. “Permeability of 13 Different Gloves to 13 Cytotoxic Agents under Controlled Dynamic Conditions.” Am J Health Syst Pharm 63(6):547–556.
38. Michaels, B, et al. 2004. “Prevention of Food Worker Transmission of Foodborne Pathogens: Risk Assessment and Evaluation of Effective Hygiene Intervention Strategies.” Food Service Technol 4(2):31–49.
39. www.food-safety.com/magazine-archive1/augustseptember-2004/understanding-the-glove-risk-paradigm-part-ii/.
40. Michaels, B. 2005. “Gloves: There’s More to It At Hand.” Food Quality Magazine Feb./March 2005:71–75.
41. King, CH. Food Safety Management: Implementing a Food Safety Program in a Food Retail Business (Springer, 2013).
42. www.fda.gov/downloads/Food/GuidanceRegulation/HACCP/UCM077957.pdf.
43. www.food-safety.com/magazine-archive1/februarymarch-2016/implementing-active-managerial-control-principles-in-a-retail-food-business/.



