
Reliably producing food product involves full knowledge and control of process hazards.[1] Employing statistical process controls to keep time and temperature, viscosity and other physical properties within upper and lower standard limits means that the processes are considered centerlined. With the food production line or food service operation running smoothly within acceptable statistical parameters, management can feel that the process is under control.[2] Don’t be fooled. There are out-of-control elements giving you a false sense of security that are potentially damaging to your process. I’m talking about food-handling gloves.
The proper use of gloves in food processing and food service is predicated on the maintenance of glove integrity.[3] Faith is placed in gloves to satisfy the twin safety objectives of protecting workers and preventing food product contamination at a reasonable cost. This is accomplished by keeping food soils and hazards associated with such soils or residues off of workers’ skin (hands), and more importantly, by keeping potential human pathogens associated with workers and their hands out of food.[4]
By definition, glove failure is a deviation away from intended control limits; otherwise, bare hands would be the norm. Foodborne pathogens reside within a variety of reservoirs, the raw food, food workers themselves, the food worker’s hands, the food worker’s family, etc. Risk is only reduced by frequent, appropriate and effective application hygiene measures, mindful of the potential for recontamination. The uses of barriers to transmission such as deli papers, utensils or gloves all have differing efficacies and limitations with respect to risk reduction. Various types of gloves are employed in the food industry, both to protect the food worker from occupational exposures related to food product or process, as well to prevent pathogen or spoilage organism transmission in from the worker to the product.[3-6]
To Glove or Not to Glove
Hand hygiene means different things to different people. Some food workers think that it means just rinsing hands under the faucet, while other workers know enough to wash, rinse and dry.[7] We know that usually less than 50% of food workers wash when necessary. A recent UK Food Standards Agency survey showed that one-third of caterers fail to wash hands after using the toilet.[8] Efficacy of a thorough hand washing sequence using antimicrobial soap, lathering well, rinsing and drying may be greater than 3-log reduction (99.9%). Combined with alcohol sanitizer treatment this can be raised even further. For example, long ago it was shown that Salmonella spp. can survive for several hours on fingertips, but that handwashing followed by hand drying with paper towels effectively reduced the risk of transmission to food.[9] If it were only that simple. There are important parts of the hand that are typically missed during the hand washing process. Thumbs, palms, spaces between fingers and fingertips, including the fingernail area, are areas where contamination is most likely to remain. The nail region presents special problems because more than 95% of hand flora resides in these areas.[10] Toilet paper poke-through results in fecal contamination of this part of the hand, commonly used hand hygiene protocols render this intervention largely ineffective, thereby additionally requiring fingernail brush use.[11-13] It is uncertain what role that the fingernail region plays in foodborne transmission of human pathogens and depending on glove strength at finger tips, whether glove use would increase or decrease the probability of transmission, when the nail region is heavily contaminated. It is known, for example, that artificial nails are linked to poor hand washing practices, more glove tears and to outbreaks.[14-15] In gloves that trap heat and moisture, the potential exists to liquefy nail contamination and release it when punctured. This brings up the importance of maintaining the glove barrier.
Glove use has been proposed as a risk reduction strategy by public health authorities.[16-17] Even though gloves have also been shown to transfer or amplify risk, the U.S. FDA believes that handwashing with soap and water or even use of alcohol hand sanitizers may not be enough to prevent transmission of viral and protozoan microorganisms via the fecal-oral route.[13,17] Herein lies the advantage of glove use. There is general agreement that food safety managers should reduce bare-hand contact when possible, especially with ready-to-eat foods. Thus, glove usage should be considered whenever utensils or deli/bakery papers don’t work efficiently. For glove use to make sense, workers must be trained to use gloves properly, but that’s just a starting point. Workers and management cannot put blind faith in glove use, but must evaluate potential for hygiene failure.
When a failure occurs, both worker and product can be compromised in several ways, dramatically increasing risks. The risk may be minor, only involving sporadic spoilage problems or a non-event, but it also can cause shelf-life or product safety to be compromised.[3] Two such failure factors are well-documented:
• A single glove hole can release tens of thousands of bacteria from overly moist internal glove surfaces.[19-21]
• Glove fragments can end up in food.[22]
If the quality assurance/quality control (QA/QC) department is expecting food handlers to change gloves when gloves are punctured, they should dream on. This is not human nature, especially if Sanitation Standard Operating Procedures (SSOPs) instruct workers to change gloves when they are physically away from the processing line.[3] This is a process out-of-control and a risk driver that can limit product shelf-life and cause sporadic product spoilage. Purchasing departments often impose a false sense of economy on top of the false sense of security provided by many glove types.
Risk aside, glove changes, walks away from the production line and handwashing involve increased labor costs and use of valuable production time. Also, occupational skin disease is one of the most frequent causes of lost time in the food industry and skin damage associated with the use of the wrong gloves for the job can result in unnecessary turnover.[23-26]
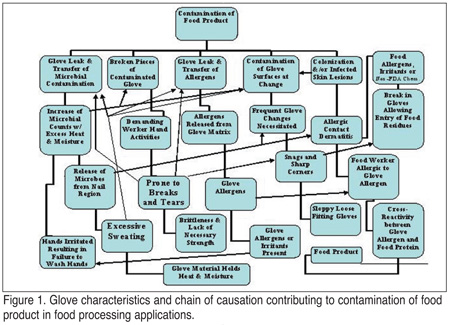 Figure 1 shows how specific glove shortcomings can result in contamination of food product in a food processing facility. Here, cumulative factors can, through a chain of causation, result in negative consequences with respect to the safety or microbial integrity of food product. A probabilistic and economic evaluation reveals that proper choice of food worker gloves can significantly impact product safety and integrity.
Figure 1 shows how specific glove shortcomings can result in contamination of food product in a food processing facility. Here, cumulative factors can, through a chain of causation, result in negative consequences with respect to the safety or microbial integrity of food product. A probabilistic and economic evaluation reveals that proper choice of food worker gloves can significantly impact product safety and integrity.
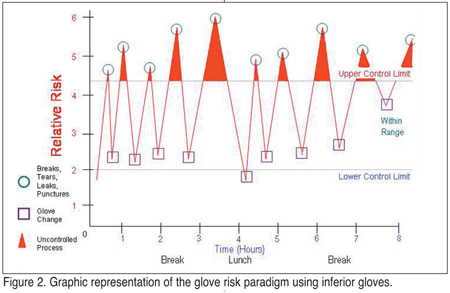 Viewed in the context of risk, Figure 2 shows that gloves that are constantly breaking or being punctured causes relative risk levels to balloon with each compromise. Here, relative risk is considered on a logarithmic scale, where each level of risk is 10 times higher than the next. Gloves are changed only after the process goes out-of-control, when a break occurs, or a worker finally decides a glove must be changed. Human nature and process line requirements cause glove changes to take place sometimes long after the damage is done, often after glove pieces have shed into food. This may take place 15 minutes or even hours after the break originally occurred, through lack of knowledge, laziness or pressures associated with the job. Pieces of glove or drips of highly contaminated human sweat can enter the product process, thereby limiting shelf-life, causing product complaints and returns, or worse, causing sporadic occurrences of foodborne illness.[18,22,27]
Viewed in the context of risk, Figure 2 shows that gloves that are constantly breaking or being punctured causes relative risk levels to balloon with each compromise. Here, relative risk is considered on a logarithmic scale, where each level of risk is 10 times higher than the next. Gloves are changed only after the process goes out-of-control, when a break occurs, or a worker finally decides a glove must be changed. Human nature and process line requirements cause glove changes to take place sometimes long after the damage is done, often after glove pieces have shed into food. This may take place 15 minutes or even hours after the break originally occurred, through lack of knowledge, laziness or pressures associated with the job. Pieces of glove or drips of highly contaminated human sweat can enter the product process, thereby limiting shelf-life, causing product complaints and returns, or worse, causing sporadic occurrences of foodborne illness.[18,22,27]
While the chart presented in Figure 2 is a representation of risk as a collection of typical events occurring to a single food worker, wearing inferior or inappropriately using gloves, it must be realized, facility-wide, risk due to damaged, leaky gloves becomes insidious. If all process line workers were plotted on the same control chart simultaneously, it would show the process as grossly out-of-control. These events might be overlooked if it occurred only a few times per shift but sadly many gloves are in a compromised state right out of the box.[4,21,28]
On average, the gloves in Figure 2 performed more or less as intended and did so within limits. Unfortunately, this thinking leads to false conclusions or optimism bias. Relative risk is not driven by averages, but is extremes driven. Outbreaks do not occur based on average sets of conditions, but by extremes of worker/product contamination.[4] In the “out-of-control” system depicted, frequent glove changes were required to maintain the façade of sanitary integrity. As described earlier, frequent glove changes are also accompanied by increase in risk. For this reason food safety experts even require glove changes to be done at some distance from the processing line. This time away from the line is costly to worker and facility productivity.
Glove Safety and Regulatory Status
The 2001 FDA Food Code recognizes that various grades of glove are available for use by food facilities and considers them to be either multi-use or single-use items. Material durability, strength, and cleanability are the key factors in distinguishing multi-use from single-use utensils. Multi-use utensils are required to be durable, nonabsorbent; and resistant to attack by corrosive facility sanitizers, having sufficient strength to withstand repeated washing/sanitizing treatments without damage, distortion or decomposition. Both multi-use and single-use glove types are required to be safe for contact with food, and rules do not allow migration of deleterious substances, colors, odors, or tastes to food.
Gloves used in contact with food are covered under Title 21 of the Code of Federal Regulations (CFR). Under 110.10 (b)(5), they are required to be maintained in clean, intact and sanitary conditions. The FDA considers it necessary for all food service and food processing gloves to be covered under 21 CFR 177.2600 for repeat contact with food items under indirect food additive regulations.[29] In order to verify FDA status under this regulatory framework, prolonged two-stage, nine-hour high temperature chemical extraction testing using water and hexane solvents is required. Using test results for this stringent testing and chemical component compliance with existing regulations, USDA/FDA status can be determined. Using this approach, your glove supplier should be able to provide a USDA/FDA letter of guarantee. A red flag should go up regarding safety and regulatory status if they are unable to do so. From manufacturers’ information provided on some of these newer glove types, food contact status is not altogether clear and must be verified.
Up until the HIV epidemic there were only a few glove types available to food establishments. There are now more than 200 different types considering material composition, thickness differences, internal treatments, powder types (if any), modulus of elasticity, and exterior coatings.[30] The vast selection of glove types on the market today was driven also in part by allergy problems with natural rubber latex in the medical field and the glove industry’s response to find suitable alternatives. There are three primary physiological reactions associated with glove sensitivity. They are as follows:
• Type I: Immediate hypersensitivity (IgE-mediated protein urticaria)
• Type IV: Allergic contact dermatitis (delayed Type I hypersensitivity)
• Irritation (irritant contact dermatitis)
Natural rubber latex is known to contain more than 35 different proteins. Both NRL allergy and these cross-reacting food allergies are described as Type I, IgE-mediated immediate hypersensitivity.[31] Clinical symptoms of natural rubber latex allergy can include rhinitis, asthma, angioedema, dysphonia, urticaria, erythema, nausea, vomiting, hypotension and anaphylaxis.[31] Many food types can cross-react with the latex allergen resulting in allergies to foods such as banana, avocado, chestnut, kiwi, tomato and potato, to name just a few. The more severe Type I reactions to latex and cross-reacting foods can be life-threatening. Many instances have been reported where latex glove-wearing food workers handled food consumed by latex-sensitive individuals, triggering severe allergic responses. The problem of glove allergies was considered to have such negative consequences that some states or localities have banned latex gloves for food handlers altogether. This problem can be minimized by purchasing the higher quality, low-allergen latex gloves. However, there have been reports of lower latex protein content to higher leakage rates.[32] Once sensitized the only solution for the individual is a latex-free glove alternative. The problem can be so severe that the American Academy of Allergy, Asthma and Immunology recommends that latex gloves not be used by food handlers, forming the basis for a 2004 Conference for Food Protection Issue for consideration (III-24).[33] The basis for some states, such as Oregon, and large healthcare organizations banning latex gloves involved reduced workers’ comp claims.[34]
Type I reactions should not be confused with chemical sensitivity dermatitis (Type IV delayed hypersensitivity) characterized by skin redness, itching, swelling and blistering. Type IV reactions are known to occur as a result of certain accelerants, antioxidants and vulcanizing agents employed widely in the glove industry. Chemicals identified as causing Type IV reactions have tended to be thiurams, carbamates and benzothiazols in latex and nitrile gloves, and bis phenol A in vinyl gloves. Irritant dermatitis is a third skin reaction also possible as a result of chemical insult. This does not involve the body’s immune response but rather, physical or chemical insult. While virtually all glove types require one or more potentially troublesome compounds, polyurethane does not require additives relying on polymer structure only. As a result, no authenticated reports of irritation or sensitization related to polyurethane Lycra have been found.
Complexity Made Simple
Gloves are an integral part of food processing environments. Resistance to a more universal use of gloves in food service has been due to the failure to perceive a protective role for gloves by management, discomfort expressed by workers due to irritation, allergy, poor fit or excessive sweating and glove failure due to damage during use.[4-5] To address these issues it has been suggested that improved glove materials may provide solutions to the problems indicated in Figure 1.
Food safety systems are layered in complexity, and to some extent, the events described in Figure 1 are hidden from view. As those who study the logic behind why systems fail know all too well, these are the ingredients for catastrophe.[35-37] In both food processing and food service, the questions that food safety managers need to ask are, What is the intrinsic potential for system failure, and what role do gloves play in preventing that failure? To what extent are the failures hidden as sporadic complaints or shelf-life problems, and if for some reason multiple parts of the system fail simultaneously, what is the catastrophic potential of such a system?
Our previous experiences with well- publicized failures tell us that on really bad days that’s exactly what can happen but in decidedly nonlinear manner.[38] The Titanic and Challenger disasters are examples of material failures in complex systems that could have been avoided if those in charge had paid heed to the warning signs and known better the limitations of the materials. In both cases, puncture and material failure were to blame. In the former case, the warnings were in the form of hazards present in the environment, and in the latter, it was elastomeric failure of a material working outside of its design limits.[35]
Part II of this article, which will appear in the next issue of Food Safety Magazine, will cover criteria for choosing the right glove for the right application.
Barry Michaels is an independent consultant to academic institutions, government, industry and non-profit organizations and a partner in the B. Michaels Group Inc., an international scientific consultancy organization. Michaels has more than 30 years’ experience in the field of infectious disease investigation, control and prevention. Previously, he worked for Georgia-Pacific in the field of personal hygiene microbiology, product safety, regulatory affairs and product development for 14 years. He recently undertook a review of the current state of glove use and materials in the food industry for Wilshire Technologies, a leading industrial glove manufacturer.
References
1. Jouve, J.L. Good Manufacturing Practice, HACCP and Quality Systems. (Lund, Baird-Parker and Gould, eds.) Aspen Publishers. 2000.
2. Campden Food and Drink Research Association. HACCP: A Practical Guide. Technical Manual 38. Chipping Campden, U.K. 1992.
3. Lelieveld, H. Hygienic Design of Factories and Equipment in the Microbiological Safety and Quality of Food. (Lund, Baird-Parker and Gould, eds.) Aspen Publishers, Gaithersburg, MD. 2000.
4. Michaels, B. Are gloves the answer? Dairy, Food & Env. Sanitation 21(6):489-492. 2001.
5. London, L, et al. Dermatoses in the canning industry–the roles of glove use and non-occupational exposures. S. Afr. Med. J. 81:612-4. 1992.
6. Michaels B, et al. Hygiene issues associated with food service potholders and oven mitts. Food Service Technology 2:81-56. 2002b.
7. De Wit, J.C. The importance of hand hygiene in contamination of foods. Antonie van Leeuwenhock 51:523-527. 1985.
8. Hovey, L. One in three caterers don’t wash hands after using lavatory, (UK) survey shows.
Food Protection Trends 23:53-4. 2003.
9. Pether, J.V.S and R.J. Gilbert. The survival of Salmonella on finger-tips and transfer of the organisms to food. J. of Hyg. 69:673-81. 1971.
10. McGinley, K.J., et al. Compositional density of microflora in the subungual space of the hand. J. of Clinical Microbiology 26:950-3. 1988.
11. Lin, C.M., et al. Influence of fingernail length and type on removing Escherichia coli from the nail regions using different hand washing interventions. J. of Food Protection 65:117. 2002.
12. Lin, C.M., et al. A comparison of hand washing techniques to remove Escherichia coli and Caliciviruses under natural or artificial fingernails. J. of Food Protection 66:2296-301. 2003.
13. Michaels, B., et al. Use limitations of alcoholic instant hand sanitizer as part of a food service hand hygiene program. Food Service Technology 3(2):71-80. 2003.
14. Toles, A. Artificial nails: are they putting patients at risk? A review of the research. J. of Pediatric Oncologic Nursing 19:164-71. 2002.
15. Lane, K.M. Outbreaks of foodborne disease in Georgia, 2000. Georgia Epid. Rpt. 17:1-3. 2002.
16. Guzewich, J.J. The anatomy of a ‘glove rule’. Environmental News Digest Fall:4-13. 1995.
17. FDA. No Bare Hand Contact. CFP 2000 Backgrounder. Washington DC. 2000.
18. Michaels B., et al. Prevention of food worker transmission of foodborne pathogens: risk assessment and evaluation of effective hygiene intervention strategies. Food Service Technology 4(2):31-49. 2004.
19. Cole, W.R. and H.R. Bernard. Inadequacies of present methods of surgical skin preparation. Archives of Surgery 89:215-22. 1964.
20. FDA. Office of Science and Technology Annual Report, Fiscal Year 2000. Calculation of Virus Transport through Barriers as a Function of Pore Geometry, pp. 23-24. 2000.
21. Guzewich, J. and M.P. Ross. FDA White Paper: Evaluation of Risks Related to Microbiological Contamination of Ready-to-eat Food by Food Preparation Workers and the Effectiveness of Interventions to Minimize Those Risks. September 1999.
22. Canadian Food Inspection Agency. HACCP Generic Model: Dried Meats (Beef Jerky). 1997. www.inspection.gc.ca/English/fssa/polstrat/haccp/jercha/jerchaie.shtml.
23. Kanerva, L., et al. Statistical data on occupational contact Urticaria. Cont. Derm. 35(4). 1996.
24. Mathias, C.G., et al. Surveillance of occupational skin diseases: a method utilizing workers’ compensation claims. Am J Ind Med 17(3). 1990.
25. U.S. Bureau of Labor Statistics. Workplace injuries and illnesses in 1997. 2000. www.bls.gov/osh_nwrl.htm.
26. U.S. Department of Health & Human Services. Healthy People 2010: Understanding and Improving Health. 2nd ed. 2000.
27. Gould, G.W. Hygienic Design of Factories and Equipment in the Microbiological Safety and Quality of Food. (Lund, Baird-Parker and Gould, eds.). Aspen Publishers, Gaithersburg, MD. 2000.
28. Leaky gloves have become infection control nightmare. Medical Post 34(1), Jan. 13, 1998.
29. FDA. Report on progress of investigation of reported allergic reactions related to Heavea natural latex products when used in contact with food. FDA CFSAN, Office of Premarket Approval and Office of Field Programs. 2002.
30. Tillotson, T. Selecting gloves. Infection Control Today, Feb. 22-29, 2000.
31. Rodriguez, M., et al. Hypersensitivity to latex, chestnut, and banana. Ann Allergy 70(1). 1993.
32. Healthcare Purchasing News. Lower latex content linked to higher glove leakage. www.findarticles.com/fc_0/m0BPC/10_24/66491832.p1/ article.jhtml. 2000.
33. Palaski, G. Latex glove prohibited. Conference for Food Protection Issue III-24. Council III Issues and Attachments. 2004.
34. Worthington, K. and Wilburn S. Latex allergy: What’s the facility’s responsibility, and what’s yours? American J. of Nursing 101(7):88. 2001.
35. Eberhart, M.E. Why Things Break: Under-standing the World by the Way it Comes Apart. Random House, New York, NY. 2003.
36. Perrow, C. Normal Accidents: Living with High -risk Technologies. Princeton Univ. Press. 1999.
37. Dorner, D. The Logic of Failure: Recognizing and Avoiding Error in Complex Situations. Metropolitan Books, New York, NY. 1996.
38. Michaels, B. and T. Ayers. Hazard analysis of the personal hygiene process. Proceedings of the 2nd National Sanitation Foundation International Conference on Food Safety. Savannah, GA. Oct. 11-13, 2000.


