
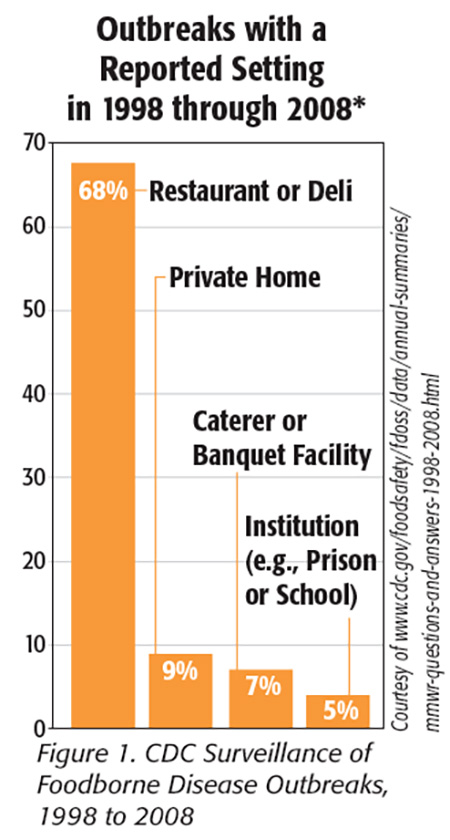
 According to the most recently published data from the U.S. Centers for Disease Control and Prevention (CDC), 88 percent of foodborne disease outbreaks in the United States between 2013 and March 26, 2015, were caused by a single food preparation location.[1] As reported in previous years (Figure 1), retail foodservice establishments were again the most commonly reported locations leading to foodborne disease outbreaks in the United States. It appears, based on numerous outbreak investigations reported in 2015, that this trend will continue. Likewise, sporadic cases of foodborne disease occur every year that are not investigated, suggesting significantly more foodborne disease cases from retail foodservice establishments than reported. Clearly, there needs to be more focus on the prevention of foodborne disease outbreaks in retail foodservice establishments, and it is the purpose of this article to help retail foodservice establishments facilitate this.
According to the most recently published data from the U.S. Centers for Disease Control and Prevention (CDC), 88 percent of foodborne disease outbreaks in the United States between 2013 and March 26, 2015, were caused by a single food preparation location.[1] As reported in previous years (Figure 1), retail foodservice establishments were again the most commonly reported locations leading to foodborne disease outbreaks in the United States. It appears, based on numerous outbreak investigations reported in 2015, that this trend will continue. Likewise, sporadic cases of foodborne disease occur every year that are not investigated, suggesting significantly more foodborne disease cases from retail foodservice establishments than reported. Clearly, there needs to be more focus on the prevention of foodborne disease outbreaks in retail foodservice establishments, and it is the purpose of this article to help retail foodservice establishments facilitate this.
A food safety management program in a retail foodservice business that is focused on the continuous identification of hazards and the implementation of food safety management systems (FSMSs) to prevent these hazards is the most important means to proactively ensure food safety in a food business (Figure 2[2]). A food safety management program, whether established in an independent restaurant or a multi-unit restaurant chain, should have multiple FSMSs and trained personnel empowered to manage operations specific to risk-based preventive controls in the supply chain and during retail foodservice operations.[2] To make the most significant impact on foodborne illness prevention, the retail foodservice establishment must achieve daily active managerial control (AMC) of the risk factors contributing to foodborne illness.
 One of the most effective FSMSs designed for retail foodservice establishments to achieve AMC is called Process Hazard Analysis and Critical Control Points (HACCP).[3] As described by the U.S. Food and Drug Administration (FDA), AMC can be achieved using an FSMS that employs specific actions or procedures to monitor and provide for immediate corrective actions of food safety hazards during retail operations. Achieving AMC is a preventive FSMS that provides a proactive rather than reactive approach to food safety through a continuous management system of monitoring, verifying and making corrections before a hazard occurs (e.g., cross-contamination of food). Process HACCP used in retail foodservice establishments is based on HACCP principles (to enable HACCP applications in a nonfood processing environment), where identified biological, chemical and physical hazards are placed under daily management to ensure that processes used to receive, store, prepare and serve foods prevent these hazards.
One of the most effective FSMSs designed for retail foodservice establishments to achieve AMC is called Process Hazard Analysis and Critical Control Points (HACCP).[3] As described by the U.S. Food and Drug Administration (FDA), AMC can be achieved using an FSMS that employs specific actions or procedures to monitor and provide for immediate corrective actions of food safety hazards during retail operations. Achieving AMC is a preventive FSMS that provides a proactive rather than reactive approach to food safety through a continuous management system of monitoring, verifying and making corrections before a hazard occurs (e.g., cross-contamination of food). Process HACCP used in retail foodservice establishments is based on HACCP principles (to enable HACCP applications in a nonfood processing environment), where identified biological, chemical and physical hazards are placed under daily management to ensure that processes used to receive, store, prepare and serve foods prevent these hazards.
A Case Study: One Incident, Two Different Outcomes
Let’s look at a simulated case study in a restaurant to discover how achieving AMC can make a significant impact on hazard management that prevents a foodborne disease outbreak.
A restaurant manager, Jessica, was cleaning a pot in the three-compartment sink in the kitchen of her new franchised barbecue restaurant when she noticed a strange woman walking through the kitchen talking to her employees. Jessica grabbed a paper towel to dry her hands and walked quickly over to intercept the woman. The stranger said, “Miss, my name is Sara, and I am the county environmental health officer. I am here to investigate a foodborne disease outbreak that your restaurant may have caused this week. We have over nine people, as of today, who have reported to the health department or went to Mercy Community Hospital because of constant vomiting, diarrhea and flu-like symptoms for the last 2 days. All of these folks claim they ate at your restaurant this week. One person who died also had similar symptoms but resided in a family care center for the elderly; not sure if she is a related case.”
Jessica said, “What? Uh, you must be kidding, right?”
“No, ma’am,” Sara said. “This looks like a norovirus outbreak due to the rapid onset of illness, an open-and-shut case, I think.” She then walked toward the hot food prep line as Jessica followed closely behind to see what she was doing.
“I just don’t know how this could have happened,” Jessica said, “I’m ServSafe certified, and we cook all of our food; it’s barbecue, how can ‘nervo’virus grow in barbecue?”
“Well, ma’am,” Sara said, “it’s a virus that doesn’t grow in barbecue like bacteria can grow, but it sure can contaminate the barbecue if one of your employees was sick or you had bad produce in your salads or another unsafe food source. It is very difficult to stop if you don’t ensure your employees are not working with these same symptoms, if you don’t have proper handwashing and/or glove-use requirements when employees are working with ready-to-eat foods like here today and if you don’t carefully ensure your ingredients come from reputable sources. Most of the time, it’s a sick employee who also doesn’t wash their hands before handling food, but it can also come in the restaurant on produce or seafood.” As Sara walked, she asked Jessica if she knew of anyone who was out sick, came to work sick or any employees or customers who might have gotten sick in the dining room, and if she could see her health policy.
“We don’t know if there are more sick people because some people don’t report their illness to the health department or visit their doctor,” Sara said, “and we likely will see more reported this and next week if this is a norovirus outbreak.”
Two different outcomes based on the absence and presence of AMC:
Without AMC: Jessica said, “I recall from my food safety manager certificate training that I needed to ask employees if they were sick and not to work, but no one looked sick this week and we were short of staff; we really needed all hands on deck, so to speak, with this holiday rush. Josh, the stock guy, did spend a lot of time in the restroom, but he said he was keeping it cleaned up regularly. I use Josh a lot on busy days to do fill-in jobs when we get busy.”
Sara didn’t look like this was helpful.
Sara looked around the kitchen and asked, “Do you require gloves when employees like Josh prepare and handle ready-to-eat foods like those barbecue sandwiches? Did Josh do any food prep this week?”
“Yeah,” Jessica said, “Josh fills in like I said, and he helped make barbecue sandwiches on the prep line twice this week due to a large catering order.”
“Do you have a handwashing requirement before they do that type of work and can you verify this?”
Jessica answered, “We talk about handwashing all the time, and we have a third-party audit once a year to verify it. We don’t allow them to wear gloves because the employees don’t wear them properly when they change tasks.”
Sara asked, “Do you have a method to ensure employees are cooking all the food at the right temperatures?” Sara checked the temperature of the pot of Brunswick stew cooking on the stovetop and took some notes on her notepad.
Sara then asked, “Can you show me the records of your produce vendors? Some of the sick people said they ate your barbecue salad too.”
Jessica looked confused and said, “We don’t have records. The produce distributor helps find us the lowest-cost produce they can find so we can reduce our food cost; you know produce goes bad quickly.”
Sara looked concerned and asked if Jessica could join her in her office. “I would recommend you close the restaurant, Jessica, at least for the rest of the week, and ensure all of your employees are well and do a deep clean and disinfection of your whole restaurant, but especially the food contact, food storage and any other surfaces that employees touch or that come into contact with food,” Sara said. “I am going to have to report this in my inspection, and it likely will be picked up by the media too. Here is a list of things you need to do immediately before you open the restaurant up again. It will help ensure that you stop the outbreak before you open back up.”
With AMC: Jessica said, “We have a health policy that requires employees to report when they get sick, and I and my other managers check each employee when they check in to work. It’s really pretty simple—we just ask them if they have had any symptoms like vomiting, fever or diarrhea, and we exclude them if we also notice anything unusual, even if they say they aren’t sick. We keep a sick log, and no one has been on the log for the past 4 weeks, but we did have a few out with the flu last month.” Jessica showed Sara the sick log. “No customers got sick in the dining room either. Oh, and I sent Josh home immediately when I noticed he was spending too much time in the restroom. When he came back after a few days, I didn’t allow him to work with food for the rest of the week.” Jessica added, “Josh is a good worker, and the only reason he is not a manager here is because he is in school and can only work part time; he even has his ServSafe certificate.”
Sara looked around the kitchen and asked, “Do you require gloves when employees like Josh prepare and handle ready-to-eat food like those barbecue sandwiches? Do you have a handwashing requirement before they do that type of work?”
Jessica answered, “We require handwashing all the time before any food prep, and all employees are required to wear blue color-coded gloves so we know they are only allowed to work with ready-to-eat foods when they have blue gloves on. In fact, we also record this every day with our daily food safety checklist self-assessment; things like blue-glove use only at the ready-to-eat food prep stations and watching them wash their hands to see if they are always doing it right. I am pretty confident that even if an employee of mine was sick and we didn’t catch it with our self-assessments, the proper handwashing and glove use would prevent it.”
Sara noticed that the hand sink in the kitchen had soap, sanitizer and a job aid to remind employees how and when to wash hands and then use a sanitizer.
Jessica said, “We also require all employees to wash their hands twice after they go to the restroom for any reason, once in the restroom and then again when they return to the kitchen before they do anything else.”
Sara asked, “Do you have a method to ensure employees are cooking all of the food at the right temperature?”
“Yeah,” Jessica said, “we use a Bluetooth thermometer and this food-check mobile app on our computer tablets to record temps after cooking every large batch of meats and stews, and every few hours at the warming line. We also check temps this way in the cooler, so we know that all the food is cooked and held properly, and we can prove it. This mobile app has really helped us track and validate that our food safety management system is working.”
“Jessica, can you show me the records of your produce vendors? Some of the sick people said they ate your barbecue salad,” Sara said.
“We only use approved brands for all our produce; matter of fact, we do this for all our foods delivered to my restaurant,” Jessica said. “Corporate makes us check the vendors and temps whenever we get deliveries. We have to reject the produce if it’s not on the approved source list, and we have to report this to Corporate. They do all the work to ensure our produce suppliers and distributors are meeting all the food safety specs. We also make sure we rinse the produce twice; once before we prep it and then again after we prep it, both times in a separate produce-only sink.”
You can quickly see that without an FSMS to achieve AMC, all the evidence points to Jessica’s restaurant as the probable cause of the outbreak. Although the health department would continue the investigation to confirm the likely source of the outbreak, the lack of AMC in Jessica’s restaurant makes it a high-risk establishment for this or future outbreaks of foodborne illness.
However, with AMC ensured by an FSMS described in part by Jessica in this case study, the likelihood of the illnesses being caused by her restaurant is very low, and it would lead the investigator to the more likely cause (e.g., if all of the customers each had consumed sushi the same week from a grocery store). The very presence and evidence of AMC significantly reduce the risk that a restaurant will be associated with the cause of the foodborne disease outbreak.
Risk Factors the FSMS Should Address
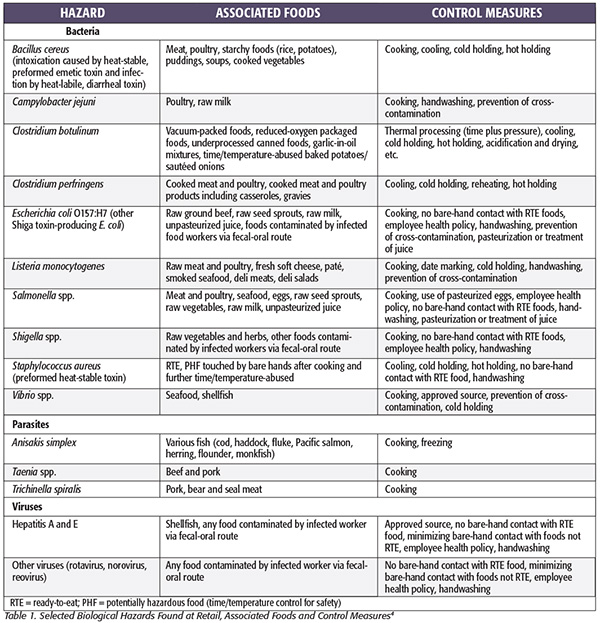 The majority of the food safety hazards that can occur in a retail foodservice establishment and their related probability (the risk) are well known. Many of the known microbiological hazards, and the best means to control them, have already been identified by FDA (Table 1[4]). Both FDA and CDC also continually study retail foodservice establishment food safety, what risk factors occur in them that lead to foodborne disease outbreaks and what methods can be used to prevent them.
The majority of the food safety hazards that can occur in a retail foodservice establishment and their related probability (the risk) are well known. Many of the known microbiological hazards, and the best means to control them, have already been identified by FDA (Table 1[4]). Both FDA and CDC also continually study retail foodservice establishment food safety, what risk factors occur in them that lead to foodborne disease outbreaks and what methods can be used to prevent them.
According to FDA,4 the top five risk factors that need to be controlled to prevent a foodborne disease outbreak are:
1. Improper hot/cold holding temperatures of potentially hazardous foods
2. Improper cooking temperatures of food
3. Contaminated utensils and equipment
4. Poor personal hygiene
5. Food from unsafe sources
Numerous additional studies performed and published in the scientific literature continue to validate these top five risk factors, and there is evidence that the lack of their control leads directly to foodborne disease outbreaks from retail foodservice establishments.[5] One study showed that certain local health department inspection violations were more likely to be associated with restaurants that had actually caused foodborne disease outbreaks in Minnesota.[6] The research showed there were recorded violations that were significantly more likely to be identified during routine inspections at restaurants that were also associated with outbreaks. When the authors compared these violations with contributing risk factors of foodborne illness as defined by CDC,[7] they found that about two-thirds of the top violations observed during inspections at outbreak-associated restaurants fell into the ‘‘contamination’’ category—for example, contamination of hands, surfaces and food.
An FSMS That Enables AMC
The best FSMS to enable AMC starts with a foundation of a written food safety plan/policy with well-defined Standard Operating Procedures (SOPs) that also lay out a clear plan of training that employees can follow to provide safe food prepared in the establishment. Employee training is critical to effective AMC, including manager-level training that enables management of the food safety plan/policy (including management of the health policy implementation) and appropriate and effective corrective actions when needed. It also must include nonmanagerial employee training at the food handler level of food safety that includes employee health policy responsibilities.
Additionally, the system should include:
• Recipe cards/step-by-step procedures posted in the kitchen that contain the specific steps for preparing a food item and the food safety critical limits, such as final cooking temperatures, that need to be monitored and verified
• Purchase specifications of all foods and a method to verify an approved source upon delivery
• Appropriate equipment and facility layout (proper flow of food prep for raw-to-ready-to-eat locations) to support the implementation of food safety procedures
• Monitoring, observing or measuring specific operational steps in the food process to determine if critical limits are being managed
• Record-keeping and documentation to verify the system is working and to use for benchmarking continuous improvement
• Ongoing quality control and assurance testing of final products (and methods to track and resolve customer complaints about food quality)
• Food safety tools to help manage compliance
• Specific goal-oriented plans, like risk control plans that outline how the restaurant will continue to control the top five foodborne illness risk factors
HACCP is the best-known method of achieving AMC of risk factors in food manufacturing/processing facilities. It is more easily implemented when the facility produces only one food product at a time on a production line that ends with the packaging of the product (i.e., where the flow of food is contained in one preparation area). In contrast, restaurants and other retail foodservice establishments produce multiple food products in the same food preparation area and often at the same time or part of the day.
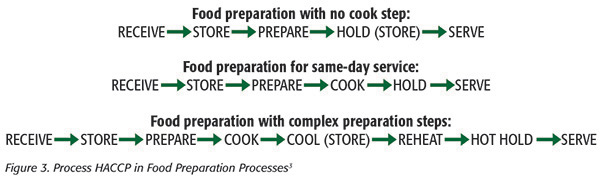 Using Process HACCP, the many variables found in food preparation of a restaurant’s menu can be divided into the three food preparation processes most often used in a retail foodservice establishment. These three processes are based on stages (activities) in the preparation of food anywhere in the restaurant kitchen or foodservice area; they have similar preventive controls and many common food preparation steps (Figure 3[3]).
Using Process HACCP, the many variables found in food preparation of a restaurant’s menu can be divided into the three food preparation processes most often used in a retail foodservice establishment. These three processes are based on stages (activities) in the preparation of food anywhere in the restaurant kitchen or foodservice area; they have similar preventive controls and many common food preparation steps (Figure 3[3]).
Not all controls in Process HACCP are CCPs but may include other control measures like physical barriers (e.g., gloves), personal hygiene controls and/or food safety procedures/tools to control the hazard. Process HACCP can be used to manage and control each of the current risk factors and should include verification of the control in place during the three food preparation processes in a retail foodservice establishment (Figure 3[3]).
For each process described in Figure 3[3], the following control measures should be included:
RECEIVE: Known safe-food source and recall preparedness, packaging to protect food, proper receiving temperature, no use-past expiration date
STORE: Proper storage temperature, location and covering when not in use, prevent cross-contamination, store away from chemicals, no use past expiration date, clean and sanitary storage containers
PREPARE: Personal hygiene, restrict or exclude sick employees, prevent cross-contamination, proper handwashing before handling foods, no bare-hand contact with ready-to-eat foods, clean and sanitary equipment, utensils, prep containers and storage containers
HOLD: Critical limit of internal temperature and heating platform to achieve it or using time alone to prevent the outgrowth and toxin production of bacteria, prevent cross-contamination, clean and sanitary storage containers
COOK: Critical limit of internal temperature and cooking platform to achieve it, clean and sanitary equipment
COOL: Critical limit of internal temperature and cooling platform to achieve it, clean and sanitary storage containers
REHEAT: Critical limit of internal temperature and heating/cooking platform to achieve it, clean and sanitary equipment
HOT HOLD: Critical limit of internal temperature and heating platform to achieve it, prevent cross-contamination, clean and sanitary storage containers
SERVE: Personal hygiene, restrict or exclude sick employees, prevent cross-contamination, no bare-hand contact with ready-to-eat foods and proper handwashing before handling food
Verifying AMC: A Job for Employees
To maximize the benefit of an FSMS, each preventive control measure should be verified and recorded (some daily and others via routine surveillance checks) by employees. Although not comprehensive here, these control measures and when they should be performed can be helpful to validate AMC of the top risk factors.
The suggested primary daily checks should include (to ensure the highest risks are controlled daily):
• Sanitizer strength in bottles and pails (used to store cloth towels) and when used to sanitize dishes
• Cooking platforms and internal temperatures of products cooked
• Hot or cold holding of food internal temperatures
• Employee health and hygiene (look, ask and take action if needed)
• Handwashing compliance observed (proper steps and when performed)
• Glove use compliance (when handling ready-to-eat foods and changing gloves at the appropriate times)
• Proper date marking, use and storage of bulk ingredients and foods to prevent prep with or serving of expired foods
• Checking temperature compliance and source of foods delivered to the establishment at the time of delivery
The suggested primary surveillance checks (to ensure the FSMS is functioning) should include:
• All recipes and SOPs are current to the menu served to customers
• Only approved suppliers’ ingredients and foods are in storage and in use within the facility
• Cleaning, sanitizing and storing dishes and utensils are performed properly
• Pest management is in place to prevent infestation
• Chemical storage is used to prevent contamination of foods
• Equipment checks and maintenance are performed to ensure food safety function and prevention of pest infestations
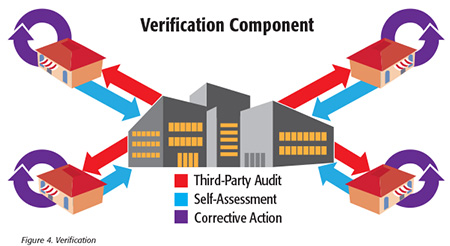 New mobile software platforms that enable use of tablets and smartphones are very valuable in the self-assessment process, especially because the software can be developed based on the establishment’s menu and food safety SOPs and the assessment of the specific control measures that should be in place. The software can also prescribe the corrective actions to take if a control measure is not in place and assign retraining to a specific employee as needed. The best means to verify an effective FSMS are via regular self-assessments performed by individual establishments and third-party audits performed by the corporation (Figure 4).
New mobile software platforms that enable use of tablets and smartphones are very valuable in the self-assessment process, especially because the software can be developed based on the establishment’s menu and food safety SOPs and the assessment of the specific control measures that should be in place. The software can also prescribe the corrective actions to take if a control measure is not in place and assign retraining to a specific employee as needed. The best means to verify an effective FSMS are via regular self-assessments performed by individual establishments and third-party audits performed by the corporation (Figure 4).
Applying AMC Principles to Chain Foodservice Establishments
The most effective means of achieving AMC in retail operations that are part of a multi-unit corporation are when the FSMS is uniformly supported by all areas of the corporation that oversee distribution and operations in each retail foodservice facility (see Figure 2[2]). Many of the corporate business functions that the FSMS supports directly enable the operations of an FSMS at the foodservice-establishment level.[2] However, the core FSMS functions must operate uniformly at each individual foodservice establishment. For example, to ensure the effectiveness of all the cost and work put into a system to ensure safe food suppliers (e.g., ingredients and raw meats, etc.), the operators must use only these approved suppliers and verify them regularly. This process also ensures the proper function of a recall program wherein the corporate business may need to alert individual foodservice operators that a food delivered to their facility should not be served. It is not within the scope of this article to discuss these important systems at the corporate level, but corporate chain foodservice businesses should have established systems within the food safety management program. Various organizations, such as the National Restaurant Association, the National Environmental Health Association, the National Council of Chain Restaurants, FDA and local and state health departments, are great sources to benchmark effective programs.
The Value Propositions of AMC for Public Health
The majority of a state or local health department’s regulatory role in food safety for the public is performed through surveillance, with an emphasis on identifying and citing food code rule violations and verifying their correction through inspections. Although it’s an important and effective FSMS employed by regulators, using this method of inspection and enforcement alone oftentimes does not result in any noticeable improvement in sustained compliance with the rules in retail foodservice establishments. This type of control of food safety risk alone can falsely lead the establishment operator to assume the health inspector will manage the risk for them (shifting responsibility) and let them know what they should and should not be doing. This system alone can also create a violator/enforcer relationship between health departments and retail foodservice operators.[8] Implementing a proactive FSMS to enable AMC can work to prevent poor health inspection scores/grades by ensuring food safety controls are active at all times (see “Value Propositions for Achieving AMC”). When a foodservice establishment performs a daily “inspection” via use of its FSMS, better health inspection scores/grades result because fewer violations are likely to occur. This process also reduces the need for additional follow-up inspections by regulators, allowing them to focus on higher-risk retail foodservice establishments that do not use an FSMS.
Evidence for this was seen using announced inspections as part of an AMC education program for retail foodservice establishments in Minnesota, reducing critical violations by one-half, which was sustained with later, unannounced inspections.[9]
When AMC is achieved in a retail foodservice establishment, microbiological hazards are also reduced. A study by Lahou et al.[10] found that during a 1-year period, when a new FSMS was implemented in a foodservice operation, there was sustained compliance with low microbial-quality metrics, hygiene indicators and presence of viable (infective) pathogens (Listeria monocytogenes, Salmonella, Bacillus cereus and Escherichia coli O157) on surfaces. Proper supplier selection and certification contributed to the reduction of the numbers of pathogens on raw foods going into the retail foodservice establishments.
Does Your Establishment Have an FSMS That Can Achieve AMC?
Use this checklist to see how close you are in the development of a formal FSMS:
• Do you have written SOPs and recipes for each product that employees are required to use for all food preparation, storage and service?
• Do you require managers in the establishment at all times who are certified?
• Are nonmanager-level employees who handle food required to go through food safety training before they work with food?
• Is your facility designed to separate raw from ready-to-eat foods for preparation with the proper handwashing stations between the two?
• Do your managers conduct self-assessments of SOPs including equipment function daily, and do they know what corrective actions are required?
• Do you require use of only approved (certified) suppliers for ingredients and foods delivered to the facility?
• Do you have a process to check the health policy, and is it functioning in the identification and exclusion of employees who might have a foodborne illness?
• Does anyone check temperatures of the cooked food and hot and cold holding of foods?
• Do you have scheduled cleaning and sanitation SOPs?
• Does the facility have regular equipment maintenance checks to ensure food equipment is working properly and does not contribute to food safety hazards?
A Challenge to All Retail Foodservice Businesses
Nearly all businesses strive to use well-trained employees and the principles of business management to lead their organizations and ensure their business is competitive and can maintain increasing profit. An FSMS and trained employees are no different and can equally ensure the business can remain competitive and increase profits by providing safe food. I would challenge each retail foodservice business, whether an independent or a franchisee of a retail chain, to work toward achieving AMC in every facility so that by the end of 2016, the CDC annual report from that year (probably to be published in 2018) will show significantly fewer foodborne disease outbreaks resulting from retail foodservice establishments in the United States. We should all work together to achieve this milestone to protect consumers and grow the retail foodservice business.
Hal King, Ph.D., is CEO, Public Health Innovations LLC, www.publichealthinnovations.biz, and a member of the Editorial Advisory Board of Food Safety Magazine. He can be reached at halking@pubhealthinnovations.com.
References
1. www.cdc.gov/foodsafety/pdfs/foodborne-disease-outbreaks-annual-report-2013-508c.pdf.
2. King, CH. Food Safety Management: Implementing a Food Safety Program in a
Food Retail Business (New York: Springer-Verlag, 2013).
3. www.fda.gov/downloads/Food/GuidanceRegulation/HACCP/UCM077957.pdf.
4. www.fda.gov/downloads/Food/FoodSafety/RetailFoodProtection/FoodborneIllnessandRiskFactorReduction/RetailFoodRiskFactorStudies/UCM224682.pdf.
5. Hedberg, CW. 2013. “Explaining the Risk of Foodborne Illness Associated with Restaurants: The Environmental Health Specialists Network (EHS-Net).” J Food Prot 76:2124–2125.
6. Petran, RL et al. 2012. “Criteria More Likely to Be Associated with Outbreak Restaurants in Minnesota.” J Food Prot 75:2007–2015.
7. Lynch, M et al. 2006. “Surveillance for Foodborne-Disease Outbreaks—United States, 1998–2002.” Morb Mortal Wkly Rep 55:1–42.
8. www.heartlandcenters.slu.edu/ephli/finalProjects09/27JanetStetzer.doc.
9. Reske, KA et al. 2007. “Beneficial Effects of Implementing an Announced Restaurant Inspection Program.” J Environ Health 69:27–34.
10. Lahou, E et al. 2012. “Microbiological Performance of Food Safety Management System in a Foodservice Operation.” J Food Prot 75:706–716.



