You hear about it every day. The headlines tell of Listeria traced to a manufacturing plant; the evening news covers a Salmonella outbreak in a national restaurant chain; a friend casually mentions her disgust after seeing a cockroach in your favorite bistro. The public focuses on the safety of the food we eat more than ever, and rightfully so. The Centers for Disease Control and Prevention (CDC) estimates that in the U.S. there are 76 million foodborne illnesses annually, resulting in 5,000 deaths.
Has a stigma developed from this increased attention to the food we eat? Consider the last time you had a stomachache. What was your first thought? Was it something along the lines of, “Where did I last eat out?” Because the media reports about outbreaks focus on restaurants and home meal replacement sources, these establishments carry the public perception of unsafe food by default. The public automatically holds foodservice establishments accountable for any instance of foodborne illness. Should some of that responsibility be placed where millions of meals are prepared and consumed each day, at home?
For decades this question remained inadequately answered. Studies on food safety practices in homes focused on consumer knowledge, not actual performance. This changed in 1997, when Audits International (A.I.) conducted its first Home Food Safety Study (HFSS). A.I. used its field force of trained auditors to evaluate the food handling practices of homes across North America. Following the same methods used in thousands of restaurant evaluations each year, A.I. sought to determine how often the public used proper safety practices as part of meal preparation.
The results were staggering; only four out of 106 participants met acceptable standards. The evaluation identified at least one critical violation (i.e. a practice that, by itself can potentially lead to illness or injury) in 96% of the participating households. Although comparable information had not been released about industry, HFSS clearly established that the public could no longer absolve themselves of responsibility for food safety.
Since the initial HFSS, Audits International has continued to promote the importance of home food safety with subsequent research. Additionally, the goal of the HFSS evolved to reflect industry trends. In 1997, the objective was to find out how often deficient food safety practices occur. Following 1997’s grim results, the basis of the 1999 study expanded beyond the frequency of violations to identifying their causes. A.I. concluded that the reason participants used unsafe food practices was due to a lack of education more often than motivation. In 2000, A.I. further enhanced the HFSS to differentiate between education and awareness because past results suggested that fully knowledgeable people did not realize they were committing unsafe practices.
In this article, the results from the third A.I. Home Food Safety survey are discussed, including the current state of home food safety, the root causes of food safety failure and a comparison to the U.S. Food and Drug Administration’s (FDA) recent baseline in various foodservice establishments.
Study Design
The 2000 HFSS included 115 households in 74 metropolitan areas. Auditors observed meal preparation, service, post-meal cleanup and handling/storage of leftovers. The inspection required approximately 60 minutes of evaluation time, generally spread over a few hours. Each auditor utilized an objective critical control point approach for home evaluation, similar to that used by A.I. in restaurants. Performance was compared to standards from the 1999 U.S. Food Code. The following issues were evaluated:
• Temperature taking practices
• Storage and rotation practices (time, temperature, expiration)
• Hot and cold ingredient preparation and holding
• Sanitation and chemical storage
• Personal practices (cross-contamination, hand-washing)
• Kitchen condition (infestation, maintenance, plumbing)
Household selection was not random. Auditors evaluated the homes of willing acquaintances who had not participated in past studies. All participants were volunteers, they probably believed they would perform well, and were better educated than the average U.S. population. Due to this design bias, households were likely to perform better than if evaluations were performed through unannounced, stratified random sampling.
Violations were categorized as critical or major. Critical violations can, by themselves, cause foodborne illness or injury. Major violations are frequently cited as contributing factors to food- borne illness. To achieve a rating of acceptable performance, a household had to receive no critical violations and no more than four major violations.
Section I: The State of Home Food Safety
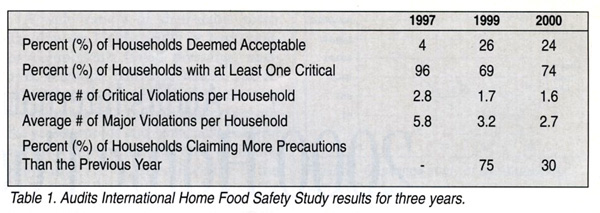 Of the 115 households evaluated, 24% met the criteria for acceptable performance. Households averaged 1.6 critical violations, with a range of zero to six. At least one critical violation was observed in 74% of the participating households. Households averaged 2.7 major violations, the total number ranging from zero to seven. Table 1 offers a comparison with past results.
Of the 115 households evaluated, 24% met the criteria for acceptable performance. Households averaged 1.6 critical violations, with a range of zero to six. At least one critical violation was observed in 74% of the participating households. Households averaged 2.7 major violations, the total number ranging from zero to seven. Table 1 offers a comparison with past results.
Since 1999, the average number of violations observed decreased slightly. However, nearly three out of four households still had at least one critical violation. The results also showed a dramatic decline in the percentage of participants claiming to take more food safety precautions than the year before (from 75% in 1999 to 30% in 2000). Over the same time span, the media has decreased negative food safety coverage. It seems likely that this decrease in media attention contributed to the lack of improvement since 1999, because participants overwhelmingly identified the media as their source of food safety information.
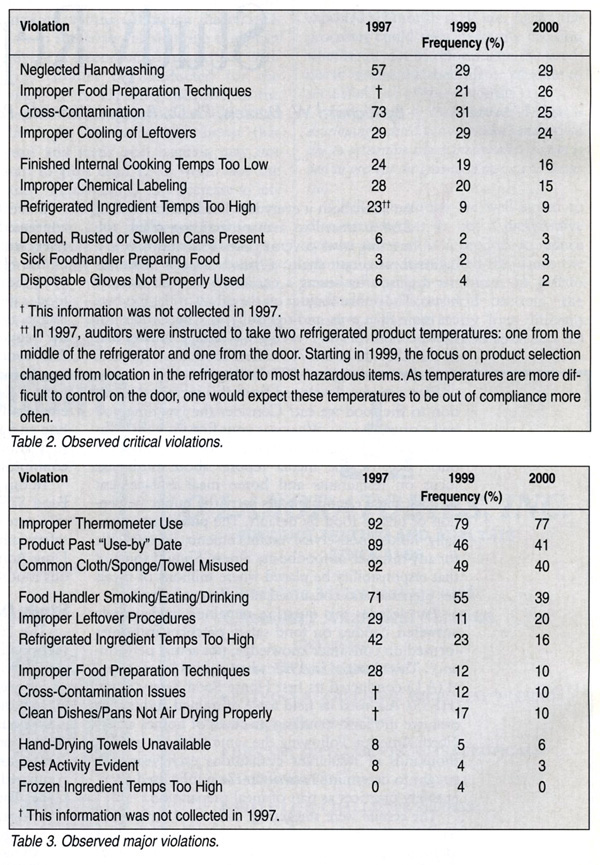
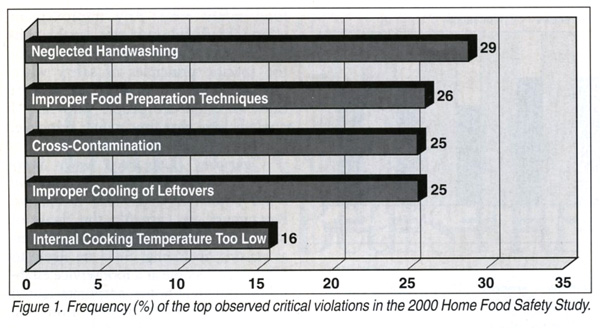 While a macroscopic view suggests little, if any, progress between the 1999 and 2000 studies, a closer look at the most frequent critical violations does suggest some advances. Specifically, the instances of cross-contamination decreased from 73% to 3 1°/o to 25°/o over the three studies, dropping from the most common violation to third. Tables 2 and 3 and Figure 1 detail home performance for each HFSS over the years.
While a macroscopic view suggests little, if any, progress between the 1999 and 2000 studies, a closer look at the most frequent critical violations does suggest some advances. Specifically, the instances of cross-contamination decreased from 73% to 3 1°/o to 25°/o over the three studies, dropping from the most common violation to third. Tables 2 and 3 and Figure 1 detail home performance for each HFSS over the years.
Section II: Education vs. Awareness vs. Motivation
The 1997 Home Food Safety Study suggested that unsafe food practices were commonplace in our homes. The 1999 study attempted to identify the reasons for violations by establishing the circumstances as educational or motivational deficiencies. In 2000, A.I. expanded the HFSS to explore the impact of awareness on food safety. The analogy that best illustrates the importance of awareness is the use of seat belts. Some people automatically put them on before starting a car. Others intend to wear seat belts but frequently forget until they’ve been driving for five to 10 minutes. The 2000 HFSS probed how often participants forgot handwashing, cross-contamination and other violations.
When auditors observed these critical violations, they asked participants if they knew they had committed a violation. The participant was then asked why the violation was committed. Auditors categorized their responses one of three ways:
• Education: Participant had never heard of the principle
• Awareness: Participant was not thinking of the principle at the time
• Motivation: Participant consciously chose to ignore the principle
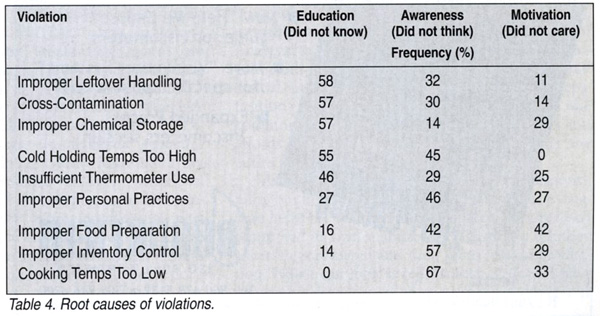 Combining all violations, 40% of the responses indicated educational factors (not knowing the food safety principle), another 40% pointed to a lack of awareness, and the remaining 20% cited motivation. However, this information is much more useful when evaluated by each violation as Table 4 and Figure 2 demonstrate. For example, in Table 4, 55% the participants receiving the “Cold Holding Temperatures Too High” violation did not know at what temperature a refrigerator should hold product. The remaining 45% were unaware their refrigerators did not hold product at the proper temperature (possibly due to the lack of a thermometer).
Combining all violations, 40% of the responses indicated educational factors (not knowing the food safety principle), another 40% pointed to a lack of awareness, and the remaining 20% cited motivation. However, this information is much more useful when evaluated by each violation as Table 4 and Figure 2 demonstrate. For example, in Table 4, 55% the participants receiving the “Cold Holding Temperatures Too High” violation did not know at what temperature a refrigerator should hold product. The remaining 45% were unaware their refrigerators did not hold product at the proper temperature (possibly due to the lack of a thermometer).
 When the study is next conducted, A.I. will more strictly qualify Education, which as defined meant, “Participant had never heard of the principle.” It was feasible for a participant who was aware that chicken needed to be cooked to a certain temperature, but did not know exactly what that temperature was, to be wrongly assigned to the Awareness category. It seems likely that this actually occurred with “Cooking Temperatures Too Low,” because not one critical violation was attributed to Education. Other critical violation attributions appear to be unaffected by this broad definition.
When the study is next conducted, A.I. will more strictly qualify Education, which as defined meant, “Participant had never heard of the principle.” It was feasible for a participant who was aware that chicken needed to be cooked to a certain temperature, but did not know exactly what that temperature was, to be wrongly assigned to the Awareness category. It seems likely that this actually occurred with “Cooking Temperatures Too Low,” because not one critical violation was attributed to Education. Other critical violation attributions appear to be unaffected by this broad definition.
Section III: Homes vs. Restaurants
 Previous A.I. Home Food Safety Studies highlighted that serious food safety concerns persist in our homes. However, the question still remained: do homes perform better than restaurants with regards to food safety? In August 2000, the FDA Retail Food Program Steering Committee released the Report of the FDA Retail Food Program Database of Foodborne Illness Risk Factors (FDA Baseline), which evaluated foodservice facilities using Food Code criteria, similar to the A.I. HFSS. The FDA Baseline (http://vm.cfsan.fda.gov/dms/retrsk.html) evaluated facilities in terms of general compliance (the percentage of evaluation points found in compliance). For example, a Quick Service Restaurant (QSR) with 42 of 50 evaluation points in compliance would receive a score of 84%. Audits International hoped to compare HFSS results to the FDA Baseline, effectively comparing homes to full and quick service restaurants, elementary schools, nursing homes, and hospitals.
Previous A.I. Home Food Safety Studies highlighted that serious food safety concerns persist in our homes. However, the question still remained: do homes perform better than restaurants with regards to food safety? In August 2000, the FDA Retail Food Program Steering Committee released the Report of the FDA Retail Food Program Database of Foodborne Illness Risk Factors (FDA Baseline), which evaluated foodservice facilities using Food Code criteria, similar to the A.I. HFSS. The FDA Baseline (http://vm.cfsan.fda.gov/dms/retrsk.html) evaluated facilities in terms of general compliance (the percentage of evaluation points found in compliance). For example, a Quick Service Restaurant (QSR) with 42 of 50 evaluation points in compliance would receive a score of 84%. Audits International hoped to compare HFSS results to the FDA Baseline, effectively comparing homes to full and quick service restaurants, elementary schools, nursing homes, and hospitals.
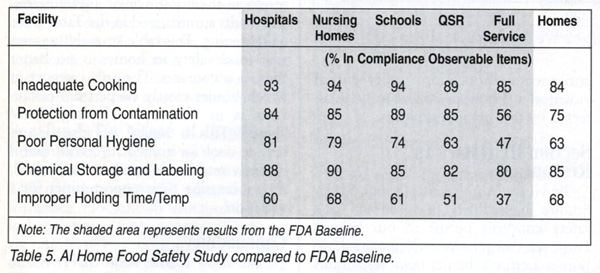
Data from the Audits International Home Food Safety Study was categorized into several food safety areas mirrored in the FDA Baseline: cooking temperatures, cross-contamination, personal hygiene, chemical storage, and time/temperature ingredient holding. The comparison with the FDA Baseline is imperfect because A.I.’s auditors answered fewer questions as “Not Observed” or “Not Applicable.” The effect of this is to slightly bias the results in the home’s favor. Nevertheless, the results summarized in the Table 5 are enlightening. This table strongly suggests that food safety in homes is no better than in restaurants. The only category in which homes clearly outperform restaurants is in “Improper Holding Time! Temp.” This is logical because homes tend to cook for immediate consumption whereas restaurants tend to hold food, thus increasing their opportunities for a violation.
Conclusions
The 2000 Home Food Safety Study yielded many fascinating results. The following conclusions are believed to be most important by Audits International:
• Despite all efforts, three-fourths of the population is still committing critical violations during meal preparation. The improvement seen between 1997 and 1999 has slowed significantly in 2000. Declining negative media attention may have contributed to this performance plateau. It is in everyone’s best interest, from the public to the regulators to industry, to make home food safety a national priority.
• Forty percent of food safety errors are attributable to a lack of education, 40% to a lack of conscious awareness, and 20% to a lack of motivation. Interestingly, these percentages vary depending on the type of food safety error. Any improvement efforts should not only educate the public, but should make them conscious of the specific principles of safety when preparing food. Fortunately, the smallest cause of errors are people who say, “I don’t believe that food safety principle. I’ve always prepared food this way.”
• Comparing Home Food Safety Study results to the FDA Baseline, it is clear that homes perform no better than restaurants. Restaurants are currently the focus of foodborne illness (FBI) reports for several reasons, including: FBIs are likely to affect more people at a foodservice establishment than at home; corporate-caused illnesses elicit more interest from the media than do home-based illnesses; and private homes are not within the jurisdiction of health departments, thus illnesses traced to homes are not pursued.
It is hoped that the results of the HFSS, when compared to the FDA Baseline, can help overcome the fallacy of blaming restaurants for all foodborne illnesses.
Richard W. Daniels, Ph.D. is founder and President of Audits International. Before starting the company he was V.P. of Nabisco/Standards Brands. For the past 30 years, Daniels has designed research in and spoken on a variety of food safety and quality issues. He received his Ph.D. in nutrition and psychology from Rutgers University. He can be reached at info@audits.com.
Brady L. Daniels is Vice President of Operations at Audits International and has been with the company since 1993. He received his M.S. in Statistics and Quality Assurance from The Georgia Institute of Technology and his B.S. in Statistical Operations and Research from the University of Illinois-Chicago.
Paul Gilmet holds a B.B.A from Loyola University-Chicago. He is a project manager at Audits International and has been with the company since 1999.
David Noonan is a Certified Food Safety Professional and holds a B.S. from the University of Illinois at Urbana-Champaign. He is a project manager with Audits International and has been with the company for five years.
Acknowledgment
Audits International thanks Ryan’s Family Steak House for their contributions to the 2000 Home Food Safety Study.
Audits International 2000 Home Food Safety Study



